Volume 32, Number 1—January 2026
Dispatch
Disseminated Nocardia ignorata Infection with Splenic and Brain Involvement in Patient with Large B-Cell Lymphoma
Cite This Article
Citation for Media
Abstract
A 79-year-old man in the United States with large B-cell lymphoma and chronic obstructive pulmonary disease had disseminated Nocardia ignorata infection involving the brain and spleen. Despite antimicrobial therapy, he died from complications. This rare manifestation highlights the need to consider Nocardia in immunocompromised patients with central nervous system and abdominal lesions.
Nocardia are filamentous, gram-positive, aerobic bacteria that infect immunocompromised hosts, causing pulmonary, cutaneous, or central nervous system disease (1–4). Dissemination to abdominal organs is rare (5). Among published cases, splenic involvement accounts for <10% of abdominal nocardiosis (5). We report disseminated N. ignorata infection with concurrent splenic and brain involvement in a patient in the United States who had large B-cell lymphoma.
Figure 1

Figure 1. Computed tomography (CT) images of brain, abdomen, and spine of 79-year-old man with chronic obstructive pulmonary disease and large B-cell lymphoma who had disseminated Nocardia ignoratainfection, United States....
A 79-year-old man with chronic obstructive pulmonary disease and large B-cell lymphoma had a new-onset seizure, left facial droop, and slurred speech. Computed tomography of the brain revealed multiple enhancing lesions with surrounding edema and mild herniation (Figure 1, panels A–E). Computed tomography of the abdominal pelvis (Figure 1, panel F, G) and chest showed a pulmonary nodule, a right renal lesion, and a 6.1-cm splenic mass.
Figure 2
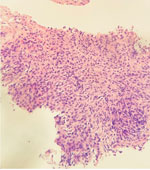
Figure 2. Ultrasound-guided biopsy image of spleen of 79-year-old man with chronic obstructive pulmonary disease and large B-cell lymphoma who had disseminated Nocardia ignoratainfection, United States. Tissue fragment shows extensive...
Figure 3

Figure 3. Brain tissue images from 79-year-old man with chronic obstructive pulmonary disease and large B-cell lymphoma who had disseminated Nocardia ignoratainfection, United States. A, B) Parenchyma with identifiable granulation...
Biopsy of the spleen demonstrated an extensively necrotic B-lymphocyte antigen cluster of differentiation 20–positive large B-cell lymphoma and limited viable tissue, explaining the negative primary stains we obtained (Figure 2). Cultures of splenic aspiration and brain biopsy grew filamentous branching N. ignorata (Figure 3). We used matrix-assisted laser desorption/ionization time-of-flight mass spectrometry for species-level identification. Blood culture results were negative. We used blood agar and chocolate agar for isolation. We extended the incubation period to accommodate slow growth.
We started the patient on antimicrobial therapy (intravenous imipenem and oral trimethoprim/sulfamethoxazole and linezolid) before susceptibility results were available. The patient’s hospital course was complicated by upper gastrointestinal bleeding. He was transitioned to comfort care and subsequently died.
Disseminated nocardiosis frequently affects the lungs, brain, or skin, but splenic involvement is rare (2,3,5). Immunosuppression from malignancy predisposes patients to opportunistic infections such as those caused by Nocardia (2,3,6). This case highlights the diagnostic challenge posed by nonspecific clinical findings and the need for microbiologic confirmation, given that Nocardia species exhibit variable antimicrobial drug susceptibility (1,3). The observed pattern of simultaneous brain and splenic involvement in the setting of lymphoma underscores the need to consider the emergence of this disease in immunocompromised patients. Our findings also support early inclusion of nocardiosis in the differential diagnosis for patients with concurrent central nervous system and visceral lesions (2,3,5,7).
Dr. Elbaz is a physician and geriatrics fellow in the Division of Geriatrics, Department of Medicine, Jacobs School of Medicine and Biomedical Sciences, University at Buffalo, Buffalo, New York, USA. He is currently a second-year nephrology fellow at HCA Houston Kingwood’s Tilman J. Fertitta Family College of Medicine, University of Houston, Houston, Texas, USA. His primary research interests include infectious diseases in older adults, immunocompromised host infections, geriatric nephrology, and onconephrology.
References
- Brown-Elliott BA, Brown JM, Conville PS, Wallace RJ Jr. Clinical and laboratory features of the Nocardia spp. based on current molecular taxonomy. Clin Microbiol Rev. 2006;19:259–82.DOIPubMedGoogle Scholar
- Minero MV, Marín M, Cercenado E, Rabadán PM, Bouza E, Muñoz P. Nocardiosis at the turn of the century. Medicine (Baltimore). 2009;88:250–61.DOIPubMedGoogle Scholar
- Beaman BL, Beaman L. Nocardia species: host-parasite relationships. Clin Microbiol Rev. 1994;7:213–64.DOIPubMedGoogle Scholar
- Tramèr L, Mertz KD, Huegli R, Hinic V, Jost L, Burkhalter F, et al. Intra-abdominal nocardiosis—case report and review of the literature. J Clin Med. 2020;9:2141.DOIPubMedGoogle Scholar
- Tajima K, Terada T, Okuyama S, Akaneya D, Hori R, Abe S, et al. Nocardia otitidiscaviarum meningitis in a diffuse large B-cell lymphoma patient with CD4-positive lymphocytopenia and persistent oligoclonal CD8-positive lymphocytes in the peripheral blood. Int J Clin Exp Pathol. 2018;11:455–61. PubMedGoogle Scholar
- Patel H, Patel B, Jadeja S, Isache C. Central nervous system nocardiosis masquerading as metastatic brain lesions. IDCases. 2019;18:
e00652 .DOIPubMedGoogle Scholar
Figures
Cite This ArticleOriginal Publication Date: January 20, 2026
Table of Contents – Volume 32, Number 1—January 2026
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Address for corresponding author: Mahmoud Ismail, Jacobs School of Medicine and Biomedical Sciences, University at Buffalo, 462 Grider St, Buffalo, NY 14215, USA
Top