Volume 7, Number 2—April 2001
THEME ISSUE
4th Decennial International Conference on Nosocomial and Healthcare-Associated Infections
Introduction
The Impact of Hospital-Acquired Bloodstream Infections
Cite This Article
Citation for Media
Abstract
Nosocomial bloodstream infections are a leading cause of death in the United States. If we assume a nosocomial infection rate of 5%, of which 10% are bloodstream infections, and an attributable mortality rate of 15%, bloodstream infections would represent the eighth leading cause of death in the United States. Because most risk factors for dying after bacteremia or fungemia may not be changeable, prevention efforts must focus on new infection-control technology and techniques.
Vital statistics outlining the major causes of death in a population are an important measure of public health. Ranking disease agents according to the number of deaths they cause can be used for strategic planning and public health resource allocation. In the United States, vital statistics support efforts to control coronary artery disease, cancer, cerebrovascular diseases, and infections (Table 1) (1). A listing of causes of death, however, provides little insight on how the diseases were acquired or managed or how they might have been prevented. Infections acquired in the hospital are an important cause of death, especially those involving the bloodstream or lung (2).
If hospital infection and death occur at high rates, we can examine the process of institutional care: access to infection control personnel, systems for prevention and early recognition, and early and appropriate therapy. With improved care, improved outcome could be anticipated. We explore the impact of hospital-acquired infections, with a focus on bloodstream infections.
Population-based surveillance studies of nosocomial infections in U.S. hospitals indicate a 5% attack rate or incidence of 5 infections per 1,000 patient-days (3–5). With the advent of managed care and incentives for outpatient care, hospitals have a concentrated population of seriously ill patients, so rates of nosocomial infections are probably correspondingly higher (6). For many larger institutions, the nosocomial infection rate may be closer to 10%.
If 35 million patients are admitted each year to the approximately 7,000 acute-care institutions in the United States, the number of nosocomial infections--assuming overall attack rates of 2.5%, 5%, or 10%--would be 875,000, 1.75 million, or 3.5 million, respectively. If 10% of all hospital-acquired infections involve the bloodstream, 87,500, 175,000, or 350,000 patients acquire these life-threatening infections each year.
Figure 1

The overall or crude rate of death does not distinguish the contribution of the patients' underlying diseases from the contribution of bloodstream infections. Recent data from the Surveillance and Control of Pathogens of Epidemiologic Importance [SCOPE] surveillance system of nosocomial bloodstream infections in U.S. hospitals identified a crude mortality rate of 27% (7), with great variation by pathogen (Figure 1).
The direct contribution of nosocomial infection, after the contribution of the underlying illnesses is accounted for, is the attributable mortality rate (8). For example, if a crude mortality rate for nosocomial candidemia of 40% is assumed (as in the SCOPE surveillance system [7]) and three-eighths of the deaths are directly due to the underlying diseases (15% of the 40%), the mortality rate attributable to candidemia would be 25% (40%-15%). Thus, candidemia would contribute five-eighths (25% of the 40%) of the crude mortality rate.
Figure 2
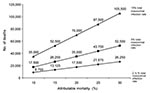
Figure 2. Estimated number of deaths caused by nosocomial infections in the United States each year. Attributable mortality rates are 10% to 30% on the X axis, and the three curves assume overall...
Several assumptions may be examined simultaneously regarding the attack rate and both crude and attributable mortality rate estimates (Figure 2). By doing so, deaths directly attributable to nosocomial bloodstream infections can be calculated, with a range of very conservative to more liberal estimates based on available data. For example, with a hospital infection rate of 5%, of which 10% are bloodstream infections, and an attributable mortality rate of 15%, 26,250 deaths can be directly linked to nosocomial bloodstream infections. However, if a 20% attributable mortality rate is assumed, the number of deaths is from 17,500 (with a 2.5% nosocomial infection rate) to 70,000 (with a 10% total nosocomial infection rate).
Figure 3
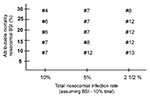
With various assumptions about total nosocomial infection rates and attributable mortality rate, the ranking of nosocomial bloodstream infections among leading causes of death can be estimated (Figure 3). This ranking reflects the total number of deaths compared with the reported numbers of leading causes of death in the United States (1). From the above estimates, if nosocomial bloodstream infections alone were counted, they would represent the fourth to thirteenth cause of death in the United States.
Figure 4
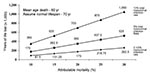
Figure 4. Years of life lost annually in the United States from nosocomial infections. Attributable mortality rates are 10% to 30% on the X axis, and the three curves assume overall nosocomial infection...
The impact of nosocomial bloodstream infections can also be examined in terms of years of life lost. SCOPE (M. Edmond, pers. comm.) indicates that the median age of patients dying of nosocomial bloodstream infections is 57 years. If these patients are 60 years of age, without bloodstream infection they would have lived to age 70. This assumption is reasonable since only attributable deaths are included in the calculations (Figure 4). As an example, if the attributable mortality rate is 20% and the total nosocomial infection rate is 5%, the total number of years of life lost in the United States would be 350,000 annually. If the attributable mortality rate were only 10%, the number of years of life lost annually would be 87,500 to 350,000, depending on the total infection rate.
The arguments above justify a major effort with substantial resources for preventing and controlling serious hospital-acquired infections. We suggest a quality assessment approach for hospital-based programs of infection control: structure, process, and outcome. The Study of the Efficacy of Nosocomial Infection Control (SENIC), published in 1985, showed that both structure (expertise) and process (surveillance, feedback and protocols) predicted lower infection rates (9). A subsequent analysis suggested that infection control programs represented one of the most cost effective of current public health efforts (10).
Access to improved infection-control technology is one of the promises at the dawn of the 21st century. Another is improved handwashing compliance associated with more attractive and accessible products. Two recent factors influencing infection control are use of antibiotic-bonded vascular catheters and access to alcohol hand-cleansing materials that improve handwashing compliance. In a multicenter study reported by Darouiche and colleagues, bloodstream infections were significantly reduced when patients received catheters bonded with rifampin and minocycline (11). Estimates of nosocomial bloodstream infections from the SCOPE database indicate that 70% occur in patients with central venous catheters (12). Furthermore, the study by Darouiche et al. showed that 90% of central venous catheter-associated infections could be prevented by antibiotic-bonded catheters. Assuming 200,000 total nosocomial bloodstream infections of which 35% are attributable to central venous catheters and assuming that 45% could be prevented with a catheter bonded with minocycline and rifampin, the number of lives saved according to varying attributable mortality rate estimates would be 4,745 to 9,450 (Table 2).
In a study of handwashing compliance by Bishoff and colleagues, handwashing frequency in a medical intensive-care unit (ICU) increased with access to an alcohol-based product (13). Previously, Doebbeling and colleagues showed that medicated soap solutions were more popular than alcohol preparations and thus were associated with reduced infection in intensive care units (14). The study by Doebbeling et al. showed that a 28% increase in handwashing frequency (with a higher volume of use of antiseptic soap) resulted in a substantial reduction in the rate of nosocomial bloodstream infections of 56/10,000 ICU admissions, by 45% for the attack rate and by 22% when incidence density was calculated (Table 3). In SCOPE, 49.4% of all nosocomial bloodstream infections occurred in intensive-care units. However, if 25%-50% of all bloodstream infections occur in intensive-care units and a 25% increase in handwashing would prevent 25% of bloodstream infections in ICUs, the number of lives saved would be 469 to 1,874, depending on assumptions of attributable death rate (Table 3). The emerging concept is that increased handwashing frequency will result in an improved outcome. Perhaps most striking is that in this selected comparison of the impact of changes in technology with changes in behavior, the former will likely be 5 to 10 times more effective, but at substantially increased cost. Neither, however, is mutually exclusive, and both need to be in place.
In summary, vital statistics list the major causes of death yet give little insight into environmental risk factors for disease or outcomes. Estimates of hospital-acquired bloodstream infections derived from the attributable mortality rate show the impact of the specific environment where many life-threatening infections occur. By modifying the institutional environment to improve hospital care and infection control, the outcomes for patients will greatly improve. Technological advances will likely have a greater impact on health than theoretical advances in behavior, such as improved handwashing frequency.
Dr. Wenzel is professor and chair of the department of internal medicine, Medical College of Virginia, Virginia Commonwealth University, Richmond, VA. Dr. Edmond is associate professor and associate chair for education in the department of internal medicine, Medical College of Virginia, Virginia Commonwealth University. He is also hospital epidemiologist at the Medical College of Virginia Hospital.
References
- National Center for Health Statistics. Vital statistics of the United States. 119th ed. Washington: U.S. Census Bureau. Statistical abstract of the United States;1999. p.99.
- Wenzel RP. The mortality of hospital-acquired bloodstream infections: need for a new vital statistic? Int J Epidemiol. 1988;17:225–7. DOIPubMedGoogle Scholar
- Broderick A, Mori M, Nettleman MD, Streed SA, Wenzel RP. Nosocomial infections: validation of surveillance and computer modeling to identify patients at risk. Am J Epidemiol. 1990;131:734–42.PubMedGoogle Scholar
- Morrison AJ Jr, Kaiser DL, Wenzel RP. A measurement of the efficacy of nosocomial infection control using the 95 percent confidence interval for infection rates. Am J Epidemiol. 1987;126:292–7.PubMedGoogle Scholar
- Wenzel RP, Osterman CA, Townsend TR, Veazey JM Jr, Servis KH, Miller LS, Development of a statewide program for surveillance and reporting of hospital-acquired infections. J Infect Dis. 1979;140:741–6. DOIPubMedGoogle Scholar
- Pittet D, Wenzel RP. Nosocomial bloodstream infection: secular trends in rates and mortality in a tertiary health care center. Arch Intern Med. 1995;155:1177–84. DOIPubMedGoogle Scholar
- Edmond MB, Wallace SE, McClish DK, Pfaller MA, Jones RN, Wenzel RP. Nosocomial bloodstream infections in United States hospitals: a three-year analysis. Clin Infect Dis. 1999;29:239–44. DOIPubMedGoogle Scholar
- Wenzel RP. Attributable mortality: the promise of better antimicrobial therapy. J Infect Dis. 1998;178:917–9. DOIPubMedGoogle Scholar
- Haley RW, Culver DH, White JW, Morgan WM, Emori TG, Munn VP, The efficacy of infection surveillance and control programs in preventing nosocomial infections in US hospitals. Am J Epidemiol. 1985;121:182–205.PubMedGoogle Scholar
- Wenzel RP. The economics of nosocomial infection. J Hosp Infect. 1995;31:79–87. DOIPubMedGoogle Scholar
- Darouiche RO, Raad II, Heard SO, Thornby JI, Wenker OC, Gabrielli A, A comparison of two antimicrobial-impregnated central venous catheters. N Engl J Med. 1999;340:1–8. DOIPubMedGoogle Scholar
- Wenzel RP, Edmond MB. The evolving technology of venous access. N Engl J Med. 1999;340:48–9. DOIPubMedGoogle Scholar
- Bischoff WE, Reynolds TM, Sessler CN, Edmond MB, Wenzel RP. Handwashing compliance by health care workers: the impact of introducing an accessible, alcohol-based hand disinfectant. Arch Intern Med. 2000;160:1017–21. DOIPubMedGoogle Scholar
- Doebbeling BN, Stanley GL, Sheetz CT, Pfaller MA, Houston AK, Annis L, Comparative efficacy of alternative handwashing agents in reducing nosocomial infections in intensive care units. N Engl J Med. 1992;327:88–93. DOIPubMedGoogle Scholar
Figures
Tables
Cite This ArticleTable of Contents – Volume 7, Number 2—April 2001
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Richard P. Wenzel, Department of Internal Medicine, Medical College of Virginia, Virginia Commonwealth University, Richmond, Virginia, USA: fax: 804-828-8100
Top