Volume 27, Number 1—January 2021
Synopsis
Aspergillosis Complicating Severe Coronavirus Disease
Cite This Article
Citation for Media
Abstract
Aspergillosis complicating severe influenza infection has been increasingly detected worldwide. Recently, coronavirus disease–associated pulmonary aspergillosis (CAPA) has been detected through rapid reports, primarily from centers in Europe. We provide a case series of CAPA, adding 20 cases to the literature, with review of pathophysiology, diagnosis, and outcomes. The syndromes of pulmonary aspergillosis complicating severe viral infections are distinct from classic invasive aspergillosis, which is recognized most frequently in persons with neutropenia and in other immunocompromised persons. Combined with severe viral infection, aspergillosis comprises a constellation of airway-invasive and angio-invasive disease and results in risks associated with poor airway fungus clearance and killing, including virus- or inflammation-associated epithelial damage, systemic immunosuppression, and underlying lung disease. Radiologic abnormalities can vary, reflecting different pathologies. Prospective studies reporting poor outcomes in CAPA patients underscore the urgent need for strategies to improve diagnosis, prevention, and therapy.
Invasive aspergillosis is frequently recognized in persons who have severe immunosuppression, especially that associated with hematologic malignancies and transplantation. It is characterized by hyphal invasion through bronchial or lower airway tissues, with potential vascular invasion and hallmark radiographic findings reflective of hemorrhage and necrosis. However, Aspergillus species cause a broader constellation of pulmonary disease, pathologically characterized by inflammatory disease in the airway and acute and chronic invasion, largely depending on host risks (1). Much recent work has focused on describing epidemiology and significance of aspergillosis occurring after severe viral infections, especially influenza and coronavirus disease (COVID-19).
Aspergillosis associated with severe influenza virus infection (influenza-associated aspergillosis, IAA) was reported in 1951, when Abbott et al. described fatal infection in a woman with cavitary invasive pulmonary aspergillosis noted on autopsy (2). Scattered reports appeared in thereafter; Adalja et al. summarized 27 cases in the literature during 1952–2011, which reported predominance after influenza A infection, associated lymphopenia, and occurring in persons of a broad age range (14–89 years), but with little underlying lung disease (3). There were increased numbers of cases reported during and after the 2009 influenza A(H1N1) pandemic (3–10). In 2016, Crum-Cianflone summarized 57 cases from literature; most (70%) were associated with H1N1 influenza (11). Invasive aspergillosis was described, with complicating tracheobronchitis noted in 15.8%. Reported cases (68/128) during 1952–2018 were summarized by Vanderbeke et al. (12).
An increased understanding of IAA emerged from large cohort studies performed after 2015. One 7-year retrospective study in intensive care units (ICUs) in Belgium and the Netherlands reported rates varying from 14% in immunocompetent persons to 31% in immunocompromised persons (13). Within the influenza-infected cohort, male sex, hematologic malignancy, high acute physiological assessment and chronic health evaluation II (APACHE II) score, and corticosteroid use were associated with IAA, whereas underlying diabetes was associated with lower risks. Cohort studies conducted in Canada, China, and Taiwan reported similar risk profiles and that incidence of disease varied according to season and viral epidemiology (14–17). Despite these data, 2 recent survey studies reported that risk recognition is poor outside of countries in Europe (18,19). Only 63% of critical care physicians responding to an international survey were familiar with IAA, and differences were notable between physicians in the United States (17%) and Europe (58%) (19). Similarly, a US Centers for Disease Control and Prevention–sponsored survey of infectious diseases practitioners reported that only 26% of 114 respondents were familiar with IAA (18).
An increased number of reports described a similar syndrome associated with severe COVID-19 (20–45). In this study, we add to this literature, report 20 additional cases from 2 centers in Spain and the United States and provide a review of literature describing the emerging entity of COVID-19–associated pulmonary aspergillosis (CAPA).
Case Series
Cases of CAPA were identified during March–June 2020 at Johns Hopkins University (Baltimore, MD, USA) and Hospital Clinic of Barcelona (Barcelona, Spain) by review of microbiologic and infectious diseases consult data, with approval of the institutional review boards of both institutions. Cases were defined as recovery of Aspergillus species from respiratory fluids (tracheobronchial secretions, sputum, bronchoalveolar lavage [BAL]) or positive (index ≥1) serum or BAL markers, identified with work-up for possible secondary pneumonia, typically clinically indicated with new fever or respiratory decompensation with new focal infiltrates on chest radiograph or computed tomography (CT) scan. Results for a Fungitell β-
Analyses
We calculated descriptive statistics for all data. These values are shown as frequencies, means (±SD), medians (with ranges), and proportions.
Characteristics of Cases
Patient-level data were compiled in cases recognized before June 2020 at Johns Hopkins Medical Center and Hospital Clinic of Barcelona (Table). Demographics mirrored those described for poor overall outcomes; advanced age and underlying diseases of hypertension and pulmonary disease predominated. Two patients had an underlying immunosuppressive disease. The most common immunosuppressing agents associated with CAPA included systemic or inhaled steroids, most frequently for adjunctive management of COVID-19 related inflammatory disease. CAPA was recognized a median of 11 days after symptom onset and 9 days after ICU admission. Most of these patients were hospitalized during stages characterized by inflammation or acute respiratory distress syndrome or afterwards, with lung injury, in the ICU and required respiratory support. Thus, WHO ordinal classifications at CAPA diagnoses were ≥5 (46).
Figure 1
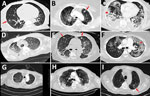
Figure 1. Representative computed tomography (CT) scans for 9 patients with aspergillosis complicating severe viral pneumonia in patients with coronavirus disease. Scans were obtained at or around diagnosis of coronavirus disease–associated pulmonary...
In cases for which CT scans were performed, radiographic reports generally described a mixture of findings attributable to the virus (ground glass opacities and crazy-paving), findings consistent with airway inflammation and mucous plugging (bronchiectasis, airway wall thickening and irregularity, bronchiectasis), and radiographic findings consistent with airway-invasive disease (consolidations, tree-in-bud nodules) (Table; Figure 1). In some cases, larger nodules with necrosis and cavitation were noted. Although nodular necrosis with cavitation was described, no radiographic reports highlighted findings that are classically associated with angioinvasive disease (ground glass attenuation described as halos) (47).
Bronchoscopy was rare, and diagnosis was most frequently supported by tracheal aspirate culture; few patients had positive serum biomarkers. Seventeen (85%) cases were identified by positive culture; most (12/17, 71%) were identified by detection of A. fumigatus. Although rarely used, results of Fungitell β-
Synopsis of Literature
Figure 2

Figure 2. Timeline of cases, series, and cohort studies reported to describe emergence of coronavirus disease–associated pulmonary aspergillosis. Reports from China are indicated according to relative times that patients were given care;...
Evidence of secondary aspergillosis developing in persons infected with severe acute respiratory syndrome coronavirus 2 was first evident in China but emphasized more clearly by case series from Europe. We provide a timeline of studies describing secondary aspergillosis occurring in persons with COVID-19, an entity that has become referred to CAPA (Figure 2) (23–45). Early reports from China noted frequent CT findings suggestive of invasive aspergillosis but provided few microbiologic or clinical details. Although without specific citation, a US Department of Defense document on COVID-19 noted that there were anecdotal communications of invasive aspergillosis documented in postmortem examinations in China (23). Use of empirical antifungal drugs was frequent; in a large study evaluating risk factors for death, »50% of persons had secondary infections, and antifungal therapy was administered in 22% (21,22). Radiographic descriptions were suggestive of invasive disease; in a study describing radiography in 51 patients, 11 (22%) had nodules with halos or reverse halos (20). Without manifestations of patient-specific data, these cohort studies nonetheless indicated that there were substantial issues with secondary fungal infections in persons who had WHO stage II–III disease. In a study from China that evaluated outcomes of persons who had increased levels of serum interleukin 6, mixed fungal infections occurred in 27.1% of 48 critically ill patients (24). In another study from China, Aspergillus species were recovered from respiratory fluids in 14% of COVID-19 patients (24).
Patient-level descriptions emerged quickly in small case series from Europe. In the first case series from Europe for COVID-19, a total of 1 of 5 patients had alveolar infiltrates on chest radiograph and Aspergillus spp. cultured from tracheal aspirate (25). Thereafter, rapid reports from centers in Austria, Belgium, France, Germany, the Netherlands, and Italy emerged (Figure 2). Differences in diagnostic methods and case definitions generated a wide degree of variability, and incidences ranged from 3.8% to 34% of persons admitted to ICUs (24–45). One center in China reported rates based on the denominator of persons hospitalized because of COVID-19 and that CAPA developed in 7% of 104 patients who had CAPA (33). Bronchoscopy was variably and infrequently performed, but frequent positive results for lavage culture, galactomannan, and Aspergillus PCR were observed, and there was visual presence of thick mucoid secretions, sometimes with evidence of bronchial inflammation, such as ulcers (33). Using multivariable analysis, Wang et al. reported that advanced age, chronic lung disease, previous positive results for the β-
Results of 3 studies that used a prospective design provided the most accurate estimates of incidence, timing, and clinical usefulness. A prospective, multicenter study that used screening with serum biomarkers and bronchoscopy for 108 mechanically ventilated patients in Italy reported that 30 (27.7%) persons met CAPA criteria (median of 4 days after ICU admission and 14 days after COVID-19 diagnosis) (38). Higher mortality rates were noted for CAPA patients than for controls; there were trends to improved survival and decreased follow-up galactomannan levels after antifungal therapy. Another study from the Netherlands applied nondirected BAL by using a closed-circuit suction catheter at a median of 2 days (range 0–8 days) after mechanical ventilation and reported 9/42 (21.4%) patients met criteria for CAPA on the basis of culture or galactomannan BAL positivity; patients with CAPA had longer duration of ICU admission (41). Finally, another prospective study that used enhanced screening with blood and respiratory samples, antigen assays (galactomannan enzyme immunoassay [GM EIA] and β-
Despite decades of case reporting and large cohort studies, many clinicians still fail to recognize that Aspergillus species can cause destructive inflammatory and invasive pathology in persons who have severe influenza, mistakenly ascribing culture results to benign airway colonization (18,19). With this in mind, the rapid recognition of CAPA, as described by reports from multiple centers (Figure 2), probably reflects previous learning and heightened awareness in centers in Europe and the clinical diligence that arises when encountering a new and unknown entity. We add 20 cases to the accumulating literature describing CAPA. Multiple pathophysiologic, clinical, and diagnostic considerations have emerged from observations reported to date.
Figure 3
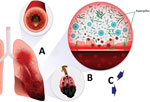
Figure 3. Schematic of coronavirus disease–associated pulmonary aspergillosis. Aspergillusconidia in airway are cleared poorly because of ≥1 defects in primary pulmonary immunity or secondary defenses, enabling conidial germination into hyphal...
First, pathophysiology of disease is distinct in this context, and not necessarily similar to invasive aspergillosis that occurs in classically immunosuppressed persons. Although it is broadly understood that Aspergillus species cause allergic manifestations, such as allergic bronchopulmonary aspergillosis, and a severe invasive pneumonia with potential angioinvasion, forms of chronic necrotizing or semiinvasive Aspergillus pulmonary disease are less well understood. These types of infections occur in persons who have more chronic immunosuppression, especially that related to prolonged steroids and chronic obstructive pulmonary disease. Common pathophysiology of these syndromes involves poor clearance of conidia, enabling bronchial inflammation and invasion, manifesting with distinct radiographic and clinical findings characteristic of airway invasion with slower development of necrosis, and exuberant and chronic tracheobronchitis, frequently with lack of angioinvasion, which limits performance of serum-based diagnostics (48). Mounting evidence suggests that severe respiratory virus infections, especially influenza and infection with severe acute respiratory syndrome coronavirus 2, can be complicated by Aspergillus airway overgrowth with pulmonary infection similarly characterized by mixed airway inflammation and bronchial invasion (Figure 3).
Distinguishing between benign airway colonization and potential disease caused by Aspergillus spp. has always been difficult because conidia are common inhabitants of airways and do not always cause inflammatory or invasive disease. To improve the process of obtaining information about what constitutes disease, early efforts have been directed toward standardizing diagnostics and definitions by using a similar approach, as for IAA, which eliminates the classic immunocompromising host criteria and relies on BAL and serum antigen results to define certainty of disease (49–51). Cases reported in this study would be considered probable CAPA if tracheal aspirate or sputum cultures met microbiologic criteria. Although more efforts are required to clarify definitions, clinicians should understand that definitions are not meant to provide clinical guidance, but to support a metric to compare epidemiology and clinical trial data. Three prospective cohort studies suggest that treatment with antifungal drugs might improve clinical outcomes (38,41,45), but definitive evidence of clinical usefulness necessitates larger comparative studies that use antifungal drugs for prevention or early therapy.
Most published studies suggest that CAPA occurs in »20%–30% of the most severely ill, mechanically ventilated COVID-19 patients (24–45). Perhaps the most accurate estimates of incidence emerged from 3 studies that deployed enhanced prospective screening and provided incidence estimates of 14%–20% and poor outcomes that might potentially be improved by use of antifungal therapy (38,41,45). Another study reported a particularly low rate of CAPA (3.8%) (40). Diagnostic differences probably contribute to variability in estimates.
Performance of diagnostic testing is variable depending on immunopathogenesis of disease. Persons who have extensive invasion into and beyond airways show positive serum GM EIA results more frequently than persons who had disease restricted to the endobronchial lumen. For this reason, sensitivity of the serum GM EIA assay is highest in hematology/oncology patients, ranging from 60% to 80%, but lower in ICU patients, estimated to be 30%–50% (48–52). In CAPA cases, serum GM EIAs have been infrequently positive. In our case series, results of β-
Despite diagnostic limitations, several studies point to utility in routine use of fungal biomarkers and early screening in persons who have COVID-19, especially directed toward BAL. Lei et al. examined residual serum samples by using a β-
Radiographic manifestations might be best understood when one considers that CAPA can be a constellation of mixed airway and invasive diseases. In our series and other reports, radiographic appearance varied from early evidence of airway inflammation and invasion (irregular airways to centrilobular nodules) to airway necrosis; this necrosis was most frequently characterized by cavitary nodules and progressive consolidation (33). Corresponding histopathology can be varied, including diffuse alveolar damage, with or without clear fungal invasion (32,43).
Although many questions linger, emerging evidence supports the conclusion that Aspergillus species cause mixed pathology in COVID-19 patients, ranging from airway inflammation to semiacute or acute bronchial invasion, similar, in most part, to that observed with severe influenza infections. Increased efforts are needed to determine the best ways to prevent, diagnose, and treat Aspergillus disease associated with COVID-19.
Dr. Marr is professor of medicine and vice chair of medicine for Innovation in Healthcare Implementation at Johns Hopkins School of Medicine, Baltimore, Maryland. Her primary research interests are fungal infections and diagnostics.
Acknowledgments
Creation of Figure 3 was supported by Cidara Therapeutics.
K.A.M. has received consultative income from Amplyx, Cidara, Merck, and Sfunga; licensing royalties from MycoMed Technologies; and research grant from Merck. C.G.-V. has received honoraria from Gilead Science, Merck, Novartis, Pfizer, Jannsen, and Lilly; and research grants from Gilead and Merck.
References
- Kosmidis C, Denning DW. The clinical spectrum of pulmonary aspergillosis. Thorax. 2015;70:270–7. DOIPubMedGoogle Scholar
- Abbott JD, Fernando HV, Gurling K, Meade BW. Pulmonary aspergillosis following post-influenzal bronchopneumonia treated with antibiotics. BMJ. 1952;1:523–5. DOIPubMedGoogle Scholar
- Adalja AA, Sappington PL, Harris SP, Rimmele T, Kreit JW, Kellum JA, et al. Isolation of Aspergillus in three 2009 H1N1 influenza patients. Influenza Other Respir Viruses. 2011;5:225–9. DOIPubMedGoogle Scholar
- Alobaid K, Alfoudri H, Jeragh A. Influenza-associated pulmonary aspergillosis in a patient on ECMO. Med Mycol Case Rep. 2019;27:36–8. DOIPubMedGoogle Scholar
- Kwon OK, Lee MG, Kim HS, Park MS, Kwak KM, Park SY. Invasive pulmonary aspergillosis after influenza a infection in an immunocompetent patient. Tuberc Respir Dis (Seoul). 2013;75:260–3. DOIPubMedGoogle Scholar
- Lat A, Bhadelia N, Miko B, Furuya EY, Thompson GR III. Invasive aspergillosis after pandemic (H1N1) 2009. Emerg Infect Dis. 2010;16:971–3. DOIPubMedGoogle Scholar
- Law P, Gelfand M, Nasser W, Shokouh-Amiri M, Boom A, Yataco J. Invasive aspergillosis in H1N1 influenza A pneumonia. Chest. 2011;140:103A. DOIGoogle Scholar
- Wauters J, Baar I, Meersseman P, Meersseman W, Dams K, De Paep R, et al. Invasive pulmonary aspergillosis is a frequent complication of critically ill H1N1 patients: a retrospective study. Intensive Care Med. 2012;38:1761–8. DOIPubMedGoogle Scholar
- Kim SH, Kim MN, Lee SO, Choi SH, Kim YS, Woo JH, et al. Fatal pandemic influenza A/H1N1 infection complicated by probable invasive pulmonary aspergillosis. Mycoses. 2012;55:189–92.
- Lee JY, Joo EJ, Yeom JS, Song JU, Yim SH, Shin DS, et al. Aspergillus tracheobronchitis and influenza A co-infection in a patient with AIDS and neutropenia. Infect Chemother. 2014;46:209–15. DOIPubMedGoogle Scholar
- Crum-Cianflone NF. Invasive aspergillosis associated with severe influenza infections. Open Forum Infect Dis. 2016;3:
ofw171 . DOIPubMedGoogle Scholar - Vanderbeke L, Spriet I, Breynaert C, Rijnders BJA, Verweij PE, Wauters J. Invasive pulmonary aspergillosis complicating severe influenza: epidemiology, diagnosis and treatment. Curr Opin Infect Dis. 2018;31:471–80. DOIPubMedGoogle Scholar
- Schauwvlieghe AFAD, Rijnders BJA, Philips N, Verwijs R, Vanderbeke L, Van Tienen C, et al.; Dutch-Belgian Mycosis study group. Invasive aspergillosis in patients admitted to the intensive care unit with severe influenza: a retrospective cohort study. Lancet Respir Med. 2018;6:782–92. DOIPubMedGoogle Scholar
- Huang L, Zhang N, Huang X, Xiong S, Feng Y, Zhang Y, et al. Invasive pulmonary aspergillosis in patients with influenza infection: A retrospective study and review of the literature. Clin Respir J. 2019;13:202–11. DOIPubMedGoogle Scholar
- Schwartz IS, Friedman DZP, Zapernick L, Dingle TC, Lee N, Sligl W, et al. High rates of influenza-associated invasive pulmonary aspergillosis may not be universal: a retrospective cohort study from Alberta, Canada. Clin Infect Dis. 2020;Jan 6:ciaa007.
- Zou P, Wang C, Zheng S, Guo F, Yang L, Zhang Y, et al. Invasive pulmonary aspergillosis in adults with avian influenza A (H7N9) pneumonia in China: a retrospective study. J Infect Dis. 2020;221(Supplement_2):S193–7. DOIPubMedGoogle Scholar
- Ku YH, Chan KS, Yang CC, Tan CK, Chuang YC, Yu WL. Higher mortality of severe influenza patients with probable aspergillosis than those with and without other coinfections. J Formos Med Assoc. 2017;116:660–70. DOIPubMedGoogle Scholar
- Toda M, Beekmann SE, Polgreen PM, Chiller TM, Jackson BR, Beer KD. Knowledge of infectious disease specialists regarding aspergillosis complicating influenza, United States. Emerg Infect Dis. 2020;26:809–11. DOIPubMedGoogle Scholar
- Thevissen K, Jacobs C, Holtappels M, Toda M, Verweij P, Wauters J. International survey on influenza-associated pulmonary aspergillosis (IAPA) in intensive care units: responses suggest low awareness and potential underdiagnosis outside Europe. Crit Care. 2020;24:84. DOIPubMedGoogle Scholar
- Li Y, Xia L. Coronavirus disease 2019 (COVID-19): role of chest CT in diagnosis and management. AJR Am J Roentgenol. 2020;214:1280–6. DOIPubMedGoogle Scholar
- Yang X, Yu Y, Xu J, Shu H, Xia J, Liu H, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respir Med. 2020;8:475–81. DOIPubMedGoogle Scholar
- Chen R, Liang W, Jiang M, Guan W, Zhan C, Wang T, et al.; Medical Treatment Expert Group for COVID-19. Risk factors of fatal outcome in hospitalized subjects with coronavirus disease 2019 from a nationwide analysis in China. Chest. 2020;158:97–105. DOIPubMedGoogle Scholar
- Matos RI, Chung KK, editors. DoD COVID-19 practice Management guide: clinical management of COVID-19. Washington (DC): Department of Health and Human Services; 2020 [cited 2020 Oct 1]. https://asprtracie.hhs.gov/technical-resources/resource/7899/dod-covid-19-practice-management-guide-clinical-management-of-covid-19
- Chen X, Zhao B, Qu Y, Chen Y, Xiong J, Feng Y, et al. Detectable serum SARS-CoV-2 viral load (RNAaemia) is closely correlated with drastically elevated interleukin 6 (IL-6) level in critically ill COVID-19 patients. Clin Infect Dis. 2020;ciaa449.
- Lescure FX, Bouadma L, Nguyen D, Parisey M, Wicky PH, Behillil S, et al. Clinical and virological data of the first cases of COVID-19 in Europe: a case series. Lancet Infect Dis. 2020;20:697–706. DOIPubMedGoogle Scholar
- Alanio A, Dellière S, Fodil S, Bretagne S, Mégarbane B. Prevalence of putative invasive pulmonary aspergillosis in critically ill patients with COVID-19. Lancet Respir Med. 2020;8:e48–9. DOIPubMedGoogle Scholar
- Koehler P, Cornely OA, Böttiger BW, Dusse F, Eichenauer DA, Fuchs F, et al. COVID-19 associated pulmonary aspergillosis. Mycoses. 2020;63:528–34. DOIPubMedGoogle Scholar
- van Arkel ALE, Rijpstra TA, Belderbos HNA, van Wijngaarden P, Verweij PE, Bentvelsen RG. COVID-19-associated pulmonary aspergillosis. Am J Respir Crit Care Med. 2020;202:132–5. DOIPubMedGoogle Scholar
- Blaize M, Mayaux J, Nabet C, Lampros A, Marcelin A-G, Thellier M, et al. Fatal invasive aspergillosis and coronavirus disease in an immunocompetent patient. Emerg Infect Dis. 2020;26:1636–7. DOIPubMedGoogle Scholar
- Prattes J, Valentin T, Hoenigl M, Talakic E, Reisinger AC, Eller P. Invasive pulmonary aspergillosis complicating COVID-19 in the ICU - A case report. Med Mycol Case Rep. 2020; Epub ahead of print. DOIPubMedGoogle Scholar
- Antinori S, Rech R, Galimberti L, Castelli A, Angeli E, Fossali T, et al. Invasive pulmonary aspergillosis complicating SARS-CoV-2 pneumonia: A diagnostic challenge. Travel Med Infect Dis. 2020;
101752 ; Epub ahead of print. DOIPubMedGoogle Scholar - Rutsaert L, Steinfort N, Van Hunsel T, Bomans P, Naesens R, Mertes H, et al. COVID-19-associated invasive pulmonary aspergillosis. Ann Intensive Care. 2020;10:71. DOIPubMedGoogle Scholar
- Wang J, Yang Q, Zhang P, Sheng J, Zhou J, Qu T. Clinical characteristics of invasive pulmonary aspergillosis in patients with COVID-19 in Zhejiang, China: a retrospective case series. Crit Care. 2020;24:299. DOIPubMedGoogle Scholar
- Meijer EF, Dofferhoff AS, Hoiting O, Buil JB, Meis JF. Buil, Meis JF. Azole-resistant COVID-19-associated pulmonary aspergillosis in an immunocompetent host: a case report. J Fungi (Basel). 2020;6:79. DOIGoogle Scholar
- Mohamed A, Hassan T, Trzos-Grzbowska M, Thomas J, Quinn A, O’Sullivan M, et al. Med Mycol Case Rep. 2020 Jun 26 [Epub ahead of print]. https://DOIGoogle Scholar
- Ghelfenstein-Ferreira T, Saade A, Alanio A, Bretagne S, Araujo de Castro R, Hamane S, et al. Recovery of a triazole-resistant Aspergillus fumigatus in respiratory specimen of COVID-19 patient in ICU - A case report. Med Mycol Case Rep. 2020; Epub ahead of print. DOIPubMedGoogle Scholar
- Santana MF, Pivoto G, Alexandre MAA, Baía-da-Silva DC, Borba MGDS, Val FA, et al. Confirmed Invasive Pulmonary Aspergillosis and COVID-19: the value of postmortem findings to support antemortem management. Rev Soc Bras Med Trop. 2020;53:
e20200401 ; Epub ahead of print. DOIPubMedGoogle Scholar - Bartoletti M, Pascale R, Cricca M, Rinaldi M, Maccaro A, Bussini L, et al.; PREDICO study group. Epidemiology of invasive pulmonary aspergillosis among COVID-19 intubated patients: a prospective study. Clin Infect Dis. 2020;
ciaa1065 ; Epub ahead of print. DOIPubMedGoogle Scholar - Nasir N, Farooqi J, Mahmood SF, Jabeen K. COVID-19-associated pulmonary aspergillosis (CAPA) in patients admitted with severe COVID-19 pneumonia: An observational study from Pakistan. Mycoses. 2020;63:766–70. DOIPubMedGoogle Scholar
- Lamoth F, Glampedakis E, Boillat-Blanco N, Oddo M, Pagani JL. Incidence of invasive pulmonary aspergillosis among critically ill COVID-19 patients. Clin Microbiol Infect. 2020;
S1198-743X(20)30412-2 ; [Epub ahead of print].PubMedGoogle Scholar - Van Biesen S, Kwa D, Bosman RJ, Juffermans NP. Detection of invasive pulmonary aspergillosis in COVID-19 with non-directed bronchioalveolar lavage. Am J Respir Crit Car Med. 2020 Jul 15 [Epub ahead of print].
- Flikweert AW, Grootenboers MJJH, Yick DCY, du Mée AWF, van der Meer NJM, Rettig TCD, et al. Late histopathologic characteristics of critically ill COVID-19 patients: Different phenotypes without evidence of invasive aspergillosis, a case series. J Crit Care. 2020;59:149–55. DOIPubMedGoogle Scholar
- Falces-Romero I, Ruiz-Bastián M, Díaz-Pollán B, Maseda E, García-Rodríguez J; SARS-CoV-2 Working Group. Isolation of Aspergillus spp. in respiratory samples of patients with COVID-19 in a Spanish Tertiary Care Hospital. Mycoses. 2020;63:1144–8; Epub ahead of print. DOIPubMedGoogle Scholar
- Helleberg M, Steensen M, Arendrup MC. Invasive aspergillosis in patients with severe COVID-19 pneumonia. Clin Microbiol Infect. 2020;
S1198-743X(20)30474-2 ; Epub ahead of print. DOIPubMedGoogle Scholar - White PL, Dhillon R, Cordey A, Hughes H, Faggian F, Soni S, et al. A national strategy to diagnose COVID-19 associated invasive fungal disease in the ICU. Clin Infect Dis. 2020;
ciaa1298 ; Epub ahead of print. DOIPubMedGoogle Scholar - World Health Organization. COVID-19 therapeutic trial synopsis, draft document. In: R&D Blueprint; 2020 [cited 2020 Sep 25]. https://www.who.int/teams/blueprint/covid-19
- Chabi ML, Goracci A, Roche N, Paugam A, Lupo A, Revel MP. Pulmonary aspergillosis. Diagn Interv Imaging. 2015;96:435–42. DOIPubMedGoogle Scholar
- Teering S, Verreth A, Peeters A, Van Regenmortel N, De Laet I, Schoonheydt K, et al. Prognostic value of serum galactomannan in mixed ICU patients: a retrospective observational study. Anaesthesiol Intensive Ther. 2014;46:145–54. DOIPubMedGoogle Scholar
- Blot SI, Taccone FS, Van den Abeele AM, Bulpa P, Meersseman W, Brusselaers N, et al.; AspICU Study Investigators. A clinical algorithm to diagnose invasive pulmonary aspergillosis in critically ill patients. Am J Respir Crit Care Med. 2012;186:56–64. DOIPubMedGoogle Scholar
- van de Groep K, Verboom DM, van de Veerdonk FL, Haas PA, van der Poll T, Schultz MJ, et al. Detection of invasive aspergillosis in critically ill patients with influenza: the role of plasma galactomannan. Am J Respir Crit Care Med. 2019;200:636–8. DOIPubMedGoogle Scholar
- Bassetti M, Giacobbe DR, Grecchi C, Rebuffi C, Zuccaro V, Scudeller L, et al.; FUNDICU investigators. Performance of existing definitions and tests for the diagnosis of invasive aspergillosis in critically ill, adult patients: A systematic review with qualitative evidence synthesis. J Infect. 2020;81:131–46. DOIPubMedGoogle Scholar
- Lahmer T, Neuenhahn M, Held J, Rasch S, Schmid RM, Huber W. Comparison of 1,3-β-d-glucan with galactomannan in serum and bronchoalveolar fluid for the detection of Aspergillus species in immunosuppressed mechanical ventilated critically ill patients. J Crit Care. 2016;36:259–64. DOIPubMedGoogle Scholar
- Lei Y, Song Y, Shu Y, Zhao Y, Huo X, Wang H, et al. Fungal antigenemia in patients with severe Coronavirus disease 2019 (COVID-19): The facts and challenges. J Microbiol Immunol Infect. 2020;53:657–9. DOIPubMedGoogle Scholar
Figures
Table
Cite This ArticleTable of Contents – Volume 27, Number 1—January 2021
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Kieren A. Marr, Johns Hopkins School of Medicine, 720 Rutland Ave, Ross 1064, Baltimore, MD 21205, USA
Top