Volume 32, Number 2—February 2026
Research
Pulmonary Complications in Fatal Yellow Fever, Brazil, 2017–2019
Figure 4
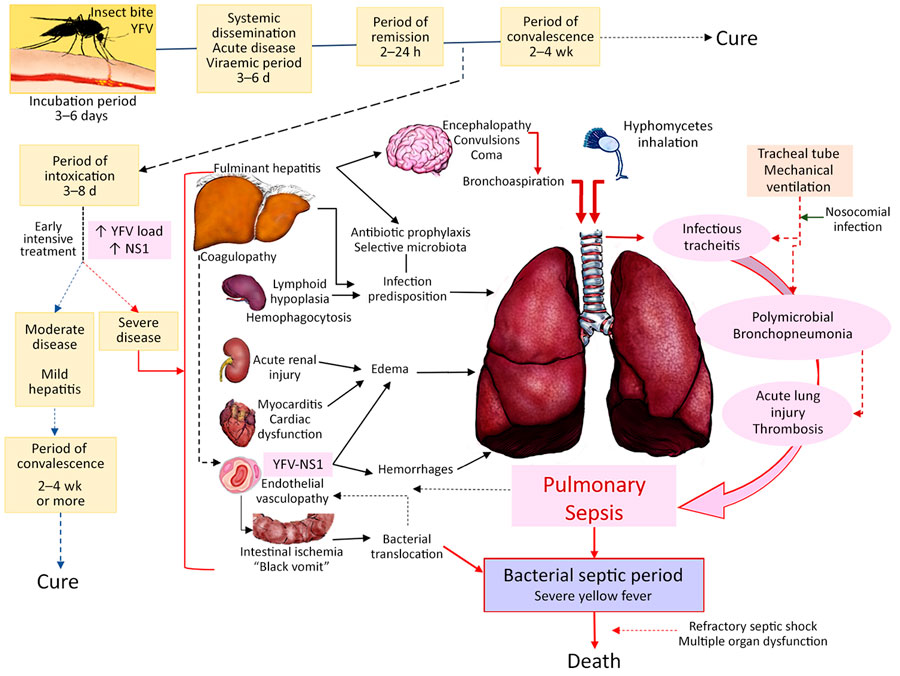
Figure 4. Proposal for the pathogenesis of respiratory tract involvement in fatal yellow fever, 2017–2019, epidemic, São Paulo, Brazil. After the mosquito bite with inoculation of YFV virions into the skin, there is a systemic spread of YFV with viremia that lasts for 5–7 days. The virus replicates in the blood, liver, spleen, kidneys, heart, brain, lungs, and other internal organs, and patients have nonspecific viral symptoms. After that is the toxemic phase, which is more severe in those with higher YFV-RNA load and higher YFV-NS1, with hepatitis, acute renal injury, immune dysfunction (lymphoid hypoplasia and hemophagocytosis), myocarditis, and systemic vascular damage. The lungs are affected in a multifactorial way. The acute liver failure due to YF-fulminant hepatitis and immune dysfunction predisposes to secondary infection. In particular, hepatic encephalopathy leads to aspiration of gastrointestinal microbiota (bacilli and Candida spp.) or inhalation of ubiquitous filamentous fungi that cause polymicrobial pneumonia and acute lung injury. The tracheal tube exerts mechanical damage to the tracheal mucosa, producing acute tracheitis associated with the aspirated flora, with ulceration and mucosal necrosis. Acute renal and myocardial dysfunction by YFV contribute to pulmonary edema. The endothelial injury also contributes to pulmonary edema which, in association with liver failure coagulopathy, leads to pulmonary hemorrhage. Acute lung injury caused by pneumonia, edema, and hemorrhage plus intestinal bacterial translocation in severe cases, presumed by evidence of intestinal ischemia and severe liver damage at autopsy, lead to bacterial sepsis, which amplifies the initial endothelial dysfunction generated by YFV, causing refractory shock and subsequent death. NS, nonstructural protein; YFV, yellow fever virus.