Volume 32, Number 6—June 2026
Dispatch
Placental Vascular Pathology Associated with Congenital Lymphocytic Choriomeningitis Virus Infection, Philadelphia, Pennsylvania, USA
Figure 1
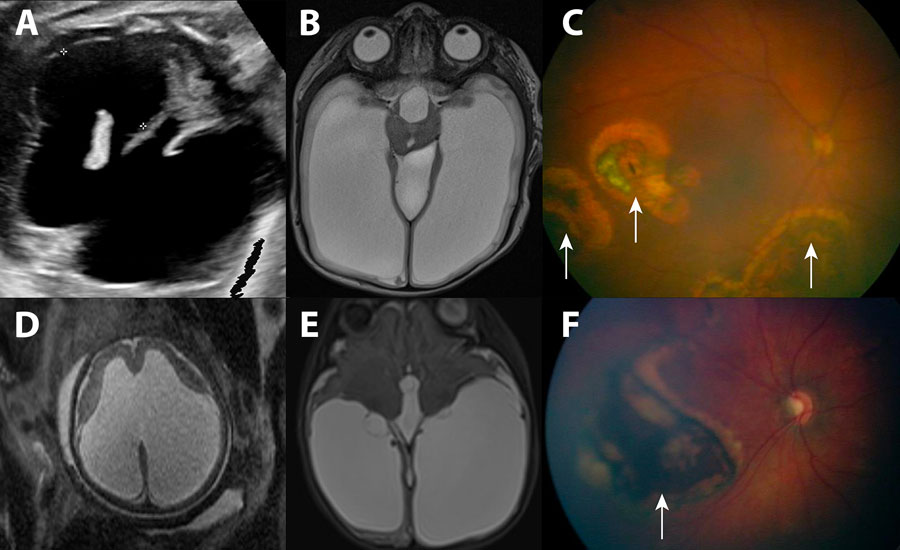
Figure 1. Imaging findings for ventriculomegaly and chorioretinitis associated with congenital lymphocytic choriomeningitis virus infection, Philadelphia, Pennsylvania, USA. A–C) Case 1; D–F) case 2. A) Routine ultrasonography at 36 weeks’ gestation, demonstrating severe cerebral ventriculomegaly in the fetus (black space between markers on the anatomic right and the unmarked black space on the anatomic left). B) Postnatal (38 weeks 4 days’ gestation) brain magnetic resonance imaging of newborn confirmed severe cerebral ventriculomegaly (large, white, fluid-filled spaces bilaterally and in the center of the image). C) Fundoscopic examination of newborn, revealing multiple areas of chorioretinitis (arrows). D) Routine ultrasonography at 36 weeks’ gestation, demonstrating severe cerebral ventriculomegaly in the fetus. E) Postnatal (38 weeks 5 days’ gestation) brain magnetic resonance imaging of newborn confirmed severe cerebral ventriculomegaly. F) Fundoscopic examination of newborn, revealing a large area of chorioretinitis (arrow).