Volume 32, Number 7—July 2026
Research Letter
Human Pulmonary Dirofilariasis, North Queensland, Australia, 20231
Cite This Article
Citation for Media
Abstract
Dirofilaria nematodes, a common cause of canine filarial disease, are increasingly recognized as emerging human pathogens. We report a case of human pulmonary dirofilariasis in the lung of a man from Northern Australia with pulmonary adenocarcinoma. This case highlights the risk for zoonotic transmission in regions with high canine heartworm prevalence.
Dirofilaria immitis is a mosquitoborne filarial nematode that causes canine filarial disease. Although this parasite primarily affects canids, human dirofilariasis caused by several canine Dirofilaria spp. nematodes are increasingly being reported, especially in Europe and Asia (1-4). Humans are accidental hosts for D. immitis nematodes and become infected after the bite of a mosquito carrying D. immitis larvae. Larvae migrate through the circulatory system and die within the pulmonary vasculature, where they infarct small vessels, leading to a surrounding pulmonary granuloma (5). Those granulomatous nodules are often diagnosed incidentally on routine chest radiography and appear as single or multiple 0.5–4.5 cm round, dense, and opaque coin lesions in the lungs, which can be mistaken for primary or metastatic pulmonary malignancy (1,5).
Human pulmonary dirofilariasis (HPD) caused by D. immitis infection is typically asymptomatic and self-limiting, and specific treatment is generally not necessary (1). Most cases of HPD are asymptomatic; wheezing, cough, hemoptysis, fever, chest pain, arthralgia, and malaise can develop (1). HPD is rarely reported (2,3), possibly underdiagnosed (3), and commonly misdiagnosed (1,3). We describe a case of HPD caused by D. immitis infection, identified incidentally in conjunction with primary pulmonary adenocarcinoma.
The male patient was 75 years of age and living in the tropical city of Townsville, Queensland, Australia; he was seen at a trauma visit in 2023. He reported a 100 pack/year smoking history, an occupational exposure to asbestos and silica, and a chronic and nonproductive cough. During his visit, imaging revealed a spiculated mass lesion measuring 35 × 28 mm in the right upper lobe that obstructed the posterior segmental bronchus and was closely associated with a separate nodule.
Figure 1
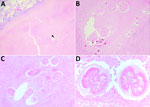
Figure 1. Dirofilaria organisms recovered from a patient with human pulmonary dirofilariasis in North Queensland, Australia, 2023. A) Degenerate D. immitisnematode (black arrow) within a necrotic human lung granuloma...
Figure 2

Figure 2. Defining anatomic features of Dirofilaria immitiswithin a small blood vessel (arteriole) in a necrotic human lung granuloma, recovered from a patient with human pulmonary dirofilariasis in Queensland, Australia,...
The patient underwent a right upper lobectomy and mediastinal lymph node sampling for suspected primary pulmonary malignancy. Histopathologic and immunohistochemical evaluation of the pulmonary nodule confirmed a 34-mm solid-predominant primary adenocarcinoma. Gross dissection of the specimen revealed an additional nodule (Figure 1). Initial findings suggested multifocal disease; microscopy of the sample revealed a helminthic co-infection. We sought consultation for helminth characterization. The morphology of the worm within the second granulomatous nodule was most consistent with D. immitis (Figure 2). No further intervention was required for the Dirofilaria infection, although the patient continued management of the lung carcinoma.
Identification of the helminthic parasite relied on characteristic morphologic features because DNA extraction and sequencing from the paraffin embedded specimen was not possible. However, D. immitis is the only canine Dirofilaria species known to occur in Australia (6,7). D. roemeri, a parasite of kangaroos and wallabies, is found in Queensland but is morphologically distinct in histological cross-sections (5,7).
Human infection remains rare in Australia; only 19 cases of D. immitis–related HPD were reported through 2012 (3), and only 1 additional case has been published since, also from North Queensland (8). A recent serosurvey of shelter dogs in Townsville revealed a high prevalence of D. immitis infection (<32%) (9), which could lead to increased zoonotic transmission.
D. immitis nematodes infect not only domestic dogs and cats but also wild canids (2). The widespread prevalence of heartworm in domestic dogs in Townsville might be attributable to dingoes (wild dogs of Australia) being common in bushland on the urban fringe of the city. Dingoes likely act as a sylvatic reservoir for infection of domestic dogs in Townsville (9). Previous necropsy surveillance studies of dingoes from the Townsville area found a heartworm prevalence of 75% (9).
We describe a case of D. immitis HPD in conjunction with primary adenocarcinoma. Similar coincidental findings of D. immitis infection and concurrent lung cancer have been previously reported in Texas, USA (6). Although those diagnoses were incidental, the overlapping clinical and radiologic features of lung cancer and pulmonary dirofilariasis pose a diagnostic challenge for clinicians and radiologists. Our report highlights the importance of preresection biopsy, meticulous gross dissection, and histologic sampling of the resection specimen for accurate diagnosis. Without those steps, the entire necrotic mass could have been included in the tumor measurement, potentially altering the tumor-nodes-metastasis stage and the associated prognosis.
Clinicians, radiologists, and pathologists practicing in regions where canine heartworm is endemic should consider HPD in the differential diagnosis of pulmonary nodules. This case adds to the limited literature describing HPD caused by D. immitis nematodes in Australia and highlights the value of a One Health approach when evaluating emerging zoonotic infections in an endemic setting.
Dr. Murray is a senior anatomical pathology trainee currently completing her specialist training with Queensland Health. Her interests include soft tissue, pulmonary, and neuropathology conditions.
References
- Saha BK, Bonnier A, Chong WH, Chieng H, Austin A, Hu K, et al. Human pulmonary dirofilariasis: a review for the clinicians. Am J Med Sci. 2022;363:11–7. DOIPubMedGoogle Scholar
- Perles L, Dantas-Torres F, Krücken J, Morchón R, Walochnik J, Otranto D. Zoonotic dirofilariases: one, no one, or more than one parasite. Trends Parasitol. 2024;40:257–70. DOIPubMedGoogle Scholar
- Simón F, Siles-Lucas M, Morchón R, González-Miguel J, Mellado I, Carretón E, et al. Human and animal dirofilariasis: the emergence of a zoonotic mosaic. Clin Microbiol Rev. 2012;25:507–44. DOIPubMedGoogle Scholar
- Colella V, Young ND, Manzanell R, Atapattu U, Sumanam SB, Huggins LG, et al. Dirofilaria asiatica sp. nov. (Spirurida: Onchocercidae)—defined using a combined morphological-molecular approach. Int J Parasitol. 2025;55:461–74. DOIPubMedGoogle Scholar
- Orihel TC, Ash LR. Parasites in human tissues. Chicago: ASCP Press; 1995.
- Mulanovich EA, Mulanovich VE, Rolston KVI. A case of Dirofilaria pulmonary infection coexisting with lung cancer. J Infect. 2008;56:241–3. DOIPubMedGoogle Scholar
- Spratt DM. Histological morphology of adult Dirofilaria roemeri and anatomy of the microfilaria. Int J Parasitol. 1972;2:193–200. DOIPubMedGoogle Scholar
- Theodore SG, Sawkins HJ, Mathew M, Yadav S, Norton R. Human pulmonary dirofilariasis: an unexpected differential diagnosis for a solitary lung lesion. Med J Aust. 2023;219:455–6. DOIPubMedGoogle Scholar
- Constantinoiu C, Croton C, Paterson MBA, Knott L, Henning J, Mallyon J, et al. Prevalence of canine heartworm infection in Queensland, Australia: comparison of diagnostic methods and investigation of factors associated with reduction in antigen detection. Parasit Vectors. 2023;16:63. DOIPubMedGoogle Scholar
Figures
Cite This ArticleOriginal Publication Date: June 25, 2026
1This case was presented at the 2024 Royal College of Pathologists of Australasia Pathology Update Conference; Adelaide, Australia; 2024 Mar 1–3.
Table of Contents – Volume 32, Number 7—July 2026
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Richard Bradbury, PHTM, Building 41, James Cook University, 1 James Cook Dr, Townsville, QLD 4814, Australia
Top