Volume 13, Number 10—October 2007
Dispatch
Malaria Diagnosis and Hospitalization Trends, Brazil
Cite This Article
Citation for Media
Abstract
We focused on rates of malaria in the state of Amazonas and city of Manaus, Brazil. Plasmodium vivax accounted for an increased number and rate of hospital admissions, while P. falciparum cases decreased. Our observations on malaria epidemiology suggest that the increased hospitalization rate could be due to increased severity of P. vivax infections.
The study of malaria prevalence in the state of Amazonas and city of Manaus indicates an increase in the percentage of hospitalized Plasmodium vivax patients and an overall increase in malaria cases caused by this parasite. Our observations on malaria epidemiology and case treatment suggest that the increased hospital admissions are associated with a higher frequency of severe disease associated with P. vivax infections. Amazonas includes most of the Brazilian Amazon Region, where malaria has been controlled but never eradicated. Since the 1980s, there has been a reemergence of malaria, which appears to coincide with changing malaria control policies associated with the ending of the Malaria Eradication Campaign (1,2).
From January through August 2003, the number of cases nationwide was reduced by 2.6%, when compared with the same period in 2002. However, this change did not represent a uniform reduction in the number of malaria infections within the country. The states of Amazonas, Rondônia, and Tocantins reported increases of 82.9%, 14.7%, and 10.3%, respectively (3). Perhaps the best indicator of what has been occurring with malaria control during the past 5 years is reflected in recent statistics for malaria in Amazonas and the city of Manaus. During the years of 2002 and 2003, the number of malaria cases reported in Amazonas increased 103.3% (4).
An observational study conducted in the reference center for diagnosis and treatment of malaria in Amazonas (Fundação de Medicina Tropical do Amazonas [FMT-AM]) described severe disease, including thrombocytopenia with hemorrhagic manifestations during infection with P. vivax. In that series, 46 (61.3%) of 75 patients admitted to the hospital for treatment of P. vivax malaria were classified with severe disease using predetermined criteria (5). We considered increased case severity as the need to hospitalize patients for treatment. Our primary goals were to present the epidemiology of malaria in Amazonas and the city of Manaus from 1980 to 2006 and to describe the overall rates, prevalence, and admission rates of malaria caused by P. falciparum and P. vivax.
We extracted total yearly cases of malaria and population size in Amazonas from the database maintained by the Brazilian Ministry of Health (DATASUS, 2004), National Foundation of Health (6–8), and Secretary of Surveillance in Health (3,9). Data from FMT-AM were extracted from the malaria logbooks (for the years before the Foundation started publishing the reports) and from the Quarterly reports (for the years that the Foundation published the reports). All malaria cases diagnosed and referred for treatment are maintained (1989–1994) and quarterly reports are published by the FMT-AM (10). Quarterly reports published from 1995 to 2004 provided the total number of malaria diagnoses, case-patients admitted to the hospital, and number of deaths. Data from 2005 and 2006 were obtained by one of the authors (M.R.F. Costa) directly at FMT-AM (Subgerência de Arquivos Médicos e Contas Hospitalares).The hospital protocol is to exclude mixed infections by additional testing. We collected and tabulated data from these sources by year, parasite species, admissions, and percent admissions (Table). Percent admission was calculated as the total number of case-patients admitted to the hospital due to the specified parasite, divided by the total number of malaria cases caused by that same parasite in FMT-AM during that year, multiplied by 100.
Figure 1
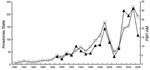
Figure 1. Malaria diagnoses (in thousands) according to blood smears positive for Plasmodium falciparum or P. vivax in Amazonas, Brazil (open squares), and Fundação de Medicina Tropical do Amazonas (FMT-AM) (solid triangles), 1980–2006.
Malaria cases from all causes in Amazonas, 1980–2006, are presented in Figure 1. An irregular increase is noted since 1988, reaching a peak in 1999, followed by a decline in 2001, only to rise again in the following years. A decrease was observed in 2006, but the data are not final. Figure 1 also shows the total number of malaria cases diagnosed at FMT-AM; fluctuations observed are very similar in direction and relative magnitude to those found statewide.
Figure 2

Figure 2. Malaria diagnoses by parasite species, Plasmodium falciparum (solid circles) and P. vivax (open circles), at the Fundação de Medicina Tropical do Amazonas (FMT-AM), Amazonas, Brazil, 1989–2006. A) Total numbers of diagnoses...
The number of infections due to P. falciparum and P. vivax diagnosed annually at FMT-AM are shown in Figure 2, panel A. The percentage of diagnosed case-patients admitted to the hospital, by parasite and year, is presented in Figure 2, panel B. In 1989, 264 (20%) of the patients with a diagnosis of P. falciparum infection were admitted to the hospital, while only 26 (0.85%) of those infected with P. vivax required admission. While P. falciparum remains the main cause of malaria admissions, we observed a significant increase in P. vivax admissions: the mean percent admissions from 1989 to 1996 was 0.59% (standard deviation [SD] 0.18), increasing to 1.91% (SD 0.74) from 1997 to 2006. This relative increase in P. vivax malaria requiring admission to the hospital for treatment was disproportionate to the change in numbers of cases and to the relative frequency of P. vivax cases over P. falciparum malaria cases.
We presented the epidemiology of recent malaria cases in the State of Amazonas and city of Manaus, emphasizing the emergence of severe P. vivax malaria. Assuming that patients requiring hospital admission were sicker than those treated as outpatients, we observed that malaria transmission in this region was continuous and fluctuated in intensity. P. vivax was consistently the main cause of malaria, but the number of patients with P. vivax requiring hospital admission increased significantly in recent years. Changes in control operations were linked to the reestablishment of malaria in major urban areas of the Amazon basin, e.g., Belém (11). In Manaus, this could have had an impact on P. vivax disease manifestations and severity but did not seem to have affected the severity of disease caused by P. falciparum, perhaps because the current policy of early diagnosis and treatment has been reported to have a greater impact on disease caused by P. falciparum than P. vivax (12,13).
In this study, we assumed that case definition and criteria for admission at FMT-AM, for both P. vivax and P. falciparum malaria, were relatively constant (http://www.fmt.am.gov.br/). Our data showed that the likelihood of hospital admissions for case-patients diagnosed with P. vivax malaria increased substantially after 1996, while the percentage of P. falciparum admissions declined. The decreasing rate of admission for P. falciparum malaria during the later years of our study supports the interpretation that the criteria for admission to FMT-AM were not loosened. It is possible that referrals to FMT-AM from elsewhere in the region increased during this period, but that would likely affect P. falciparum admissions too. Based on these considerations, we interpret the data as suggestive of an increased illness associated with P. vivax infections in the region.
In this study we did not attempt to describe the specific disease manifestations that were the basis for admissions of individual patients. However, recent reports described a range of unusual manifestations of P. vivax infection elsewhere (14), consistent with the disease manifestations reported in Manaus (5).
Biologic aspects of the human host, vector, and parasite and changes in the environment contribute to the epidemiology of malaria. Our data demonstrate that malaria is a growing health burden in the Amazon Region of Brazil and that disease caused by P. vivax is a substantial and increasing threat to the health of the population in Manaus. More studies are needed to understand the complex mechanisms of this disease and its impact on susceptible populations.
Acknowledgments
This research was supported, in part, by National Institutes of Health grants U01 AI054777 and R01 AI49726.
Dr Santos-Ciminera is originally from Brazil, where she worked at the Foundation of Tropical Medicine of Amazonas. She is currently an adjunct professor at Villa Julie College in Maryland. Her primary research interests are malaria epidemiology (traditional and molecular) and pathogenic mechanisms of infectious diseases.
References
- Brazil: Ministério da Saúde, Fundação Nacional de Saúde (FUNASA). Vigilância Epidemiológica: Programa Nacional de Prevenção e Controle da Malária–PNCM. Brasília-DF. Dec 2002. [cited 2007 Aug 29]. Available from http://www.funasa.gov.br
- Loiola CCP, da Silva CJM, Tauil PL. Controle da malaria no Brasil: 1965–2001. Rev Panam Salud Publica. 2002;11:235–44. DOIPubMedGoogle Scholar
- Brasil, Ministério da Saúde, Secretaria de Vigilância em Saúde (SVS). Boletim Epidemiológico da Malária. No. 2. Dec 2003. [cited 2007 Aug 29]. Available from http://dtr2001.saude.gov.br/svs/epi/malaria/pdfs/be_malaria_02_2003.pdf
- Fundação de Medicina Tropical do Amazonas (FMT–AM), 2005. Informe Epidemiológico, No. 1. 2005. Malária notificada no Amazonas no Período de 2003 a 2004.
- Alecrim MGC. Estudo Clínico, resistência e polimorfismo parasitário na malária pelo Plasmodium vivax, em Manaus. Brasília-DF: 2000. Universidade de Brasília; Faculdade de Medicina/Núcleo de Medicina Tropical, Tese de Doutorado. p. 177.
- Brazil: Fundação Nacional de Saúde (FUNASA). Vigilância Epidemiológica: Situação da Prevenção e Controle das Doenças Transmissíveis no Brasil. Brasília-DF. Sep 2002:22–3. [cited 2007 Aug 29]. Available from http://www.funasa.gov.br
- Brazil: Fundação Nacional de Saúde (FUNASA). Vigilância Epidemiológica. Brasília-DF. 2004. [cited 2007 Aug 29]. Available from http://www.funasa.gov.br
- Brasil: Fundação Nacional de Saúde (FUNASA). Vigilância Epidemiológica: Casos confirmados, segundo o período de diagnóstico e local de residência, por U.F. Brasil, 1980–2001. Brazil-DF. 2003. [cited 2007 Aug 29]. Available from http://www.funasa.gov.br
- Brasil: Secretaria de Vigilância em Saúde (SVS). Série histórica de casos de Doenças de Notificação compulsória-Amazonas, 1980–2001. Brasília-DF. 2004. [cited 2007 Aug 29]. Available from http://dtr2001.saude.gov.br/svs/epi/situacao doencas/transmissiveis00.htm
- Fundação de Medicina Tropical do Amazonas (FMT–AM). Boletim trimestral, Números I a X. Manaus, Amazonas, Brasil: 1995 to 2004.
- Libonati RM, Dos Santos MVN, Pinto AYN, Calvosa AM, Ventura PHM, Figueiredo JM, Malária autoctone na Grande Belém: panorama atual e prevalência no últimos seis anos. Rev Soc Bras Med Trop. 2000;33(Suppl 1):347.PubMedGoogle Scholar
- Mendis K, Sina BJ, Marchesini P, Carter R. The neglected burden of Plasmodium vivax malaria. Am J Trop Med Hyg. 2001;64:97–106.PubMedGoogle Scholar
- Pan American Health Organization. Situation of malaria programs in the Americas. Epidemiol Bull/PAHO. 2001;22:10–4.
- Kochar DK, Saxena V, Singh N, Kochar SK, Kumar SV, Das A. Plasmodium vivax malaria. Emerg Infect Dis. 2005;11:132–4.PubMedGoogle Scholar
Figures
Table
Cite This ArticleTable of Contents – Volume 13, Number 10—October 2007
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Patricia D. Santos-Ciminera, Department of Preventive Medicine and Biometrics, Uniformed Services University of the Health Sciences, 4301 Jones Bridge Rd, Room A3079, Bethesda, MD 20814, USA;
Top