Volume 15, Number 9—September 2009
Research
Chicken Consumption and Use of Acid-Suppressing Medications as Risk Factors for Campylobacter Enteritis, England
Cite This Article
Citation for Media
Abstract
In a case–control study of Campylobacter spp. risk factors in England during 2005–2006, we identified recent consumption of commercially prepared chicken as an important risk factor. The risk for illness associated with recent chicken consumption was much lower for persons who regularly ate chicken than in those who did not, which suggests that partial immunologic protection may follow regular chicken preparation or consumption. Chicken-related risk factors accounted for 41% of cases; acid-suppressing medication, for 10%; self-reported past Campylobacter enteritis, 2%; and recent acquisition of a pet dog, 1%. Understanding the risks associated with chicken from different sources will benefit strategies to reduce Campylobacter infections. Better characterization of immune correlates for Campylobacter infection is necessary to assess the relative importance of immunity and behavioral factors in determining risk.
Campylobacter spp. are the most common bacterial cause of enteritis in England. More than 40,000 cases are reported annually (1). Incidence of cases reported nationally is ≈80 per 100,000 population, but the community incidence is ≈7× higher (2). Previously identified risk factors for Campylobacter enteritis include international travel; ingestion of poultry, red meat, unpasteurized milk, and untreated water; contact with pets and farm animals; use of antimicrobial drugs and acid-suppressing medication; and diabetes (3–11).
Numerous studies implicate chicken consumption as an important risk factor for Campylobacter enteritis (6–18). However, some studies report associations specifically with eating undercooked chicken (5,6,12); others, with any type of chicken; and in 1 study, chicken consumption appeared to be protective (19). Other studies have found increased risks only with consumption of commercially prepared chicken (6–8,11,14,20).
One explanation for these disparities is that studies generally measure the average increase in risk from chicken consumption, without accounting for differences in individual susceptibility. We hypothesized that the frequency of chicken consumption modifies risk for Campylobacter enteritis associated with recent chicken consumption, possibly because persons who regularly eat chicken develop partial immunity to Campylobacter infection or because they have different consumption or preparation behaviors that influence risk for infection. We report the results of a multicenter case-control study in England designed to investigate food and other risk factors for reported Campylobacter enteritis.
Study Participants
Cases were laboratory-confirmed Campylobacter spp. infections in persons >18 years of age reported to 1 of 5 English Health Protection Units (HPUs) (East Midlands North, Cheshire and Merseyside, Cumbria and Lancashire, North East and Central London, and Essex) from April 1, 2005, through June 30, 2006. We randomly selected 5 controls per case from records of all persons registered with primary care clinics in the area. Controls were stratum-matched to cases by HPU, age group (18–34, 35–54, and >55 years), sex, and month of report.
Exclusion criteria were international travel in the 14 days before illness for case-patients (or questionnaire completion for controls) and preexisting irritable bowel syndrome. Household clusters were identified by surname and postal address; only the first case in household clusters was included. Controls reporting gastrointestinal symptoms in the preceding 14 days also were excluded.
Case and Control Recruitment
We recruited case-patients by mail through their local Environmental Health Department or HPU and asked them to return a postage-paid self-completed risk factor questionnaire. We recruited controls by mail through the Health Protection Agency Centre for Infections and asked them to complete a similar questionnaire. Reminders were sent to nonresponders after 2 and 3 weeks. Signed, informed consent was obtained from participants.
Data Collection
We inquired about demographic information, clinical details, and risk factors in the 5 days before illness for cases and questionnaire completion for controls (i.e., 5-day factors). We also collected information about routine exposures (i.e., habitual factors).
Statistical Analysis
Risk factors were grouped under 7 domains: health, occupation, pets, water, recreational exposures, food, and household details. We analyzed data by unconditional logistic regression by using Stata 8.2 software (Stata Corporation, College Station, TX, USA). ORs and 95% confidence intervals (CIs) were calculated for each exposure. Analyses were adjusted for age group (18–24, 25–34, 35–44, 45–54, 55–64, and >65 years), sex, study site, and calendar month.
We powered our study to detect an odds ratio (OR) of 1.4 for chicken consumption in the previous week (87% population prevalence (21), power = 0.8, α = 0.05), or an OR of 2.4 for an exposure with 1% prevalence.
Final Multivariable Model
Within each exposure domain, we first constructed a model comprising all habitual exposures. This model was simplified by using backward stepwise elimination until all remaining variables yielded likelihood ratio (LR) test results of p<0.05. This process was repeated for 5-day exposure variables and conducted separately for each exposure domain.
Next, we fitted a model comprising all habitual variables identified in the domain-specific regressions and simplified by backward stepwise elimination as before. A model for all 5-day exposures identified in the domain-specific regressions was similarly constructed.
Lastly, all habitual and 5-day factors from the above regressions were included in 1 model and the final model obtained by backward stepwise elimination. For all risk factors positively associated with disease, we also calculated the proportion of cases attributable to each risk factor (population-attributable fraction).
Chicken Consumption (Interaction Model)
We investigated further whether regular consumption of chicken modified the risk for disease from recent chicken consumption. We classified participants according to whether they 1) regularly ate chicken (at least once a week) and 2) had eaten it in the previous 5 days. We further classified persons who had eaten chicken in the previous 5 days according to whether they ate it in their own or someone else’s home, at a commercial establishment, or both. We fit a model with an interaction between these variables to investigate how the risk for disease varied in these subgroups relative to persons not exposed to chicken (defined as reporting they did not regularly eat chicken and had not eaten it in the previous 5 days). We assessed statistical evidence for the interaction using the LR test. In a separate model, we additionally adjusted for all other risk factors identified in the multivariable analysis. Because of small numbers in some subgroups, this latter analysis could be performed only for persons who regularly ate chicken and reported eating it in the previous 5 days.
Sensitivity Analysis
For each of the final multivariable and interaction models, we conducted 2 sensitivity analyses. First, we repeated the analysis excluding case-patients for whom the delay between symptoms onset and questionnaire completion was longer than the median delay for all case-patients. We compared the ORs from this model to those from the model comprising all case-patients to explore potential effects of differential reporting of risk factors among late responders. In the interaction model, we could perform this analysis only for persons who regularly ate chicken and reported eating it in the previous 5 days because of small numbers in other subgroups.
Second, by using an inverse probability-weighted approach (22), we investigated whether differences between participants and nonparticipants influenced results. We calculated individuals’ probabilities of participation from a 2-level random intercept logistic model regressing study participation against study site; a 3-way interaction between case and control status, age group, and sex; and area-level deprivation. To account for differences in area-level deprivation, we linked individuals’ postcodes to super output areas (SOAs), geographic boundaries comprising ≈1,000 residents for which aggregated census data are available. SOAs are ranked according to the Index of Multiple Deprivation (23), which scores SOAs on 7 domains related to unemployment, income, education, housing, living environment, crime, and healthcare access. We modeled area-level deprivation using SOA as a latent, random intercept variable at the higher level. We then used the inverse probabilities of participation from this model as weights in the final multivariable and interaction models, effectively giving more weight to persons in strata with low participation. We compared the ORs from the weighted and unweighted models to assess potential participation bias.
Ethical Approval
This study received a favorable ethical opinion from the North West Multicentre Research Ethics Committee. Approval was obtained from local research management and governance departments serving each study site.
A total of 2,381 (46.5%) case-patients and 5,256 (37.3%) controls returned questionnaires. Participants were excluded for the following reasons: missing age information (2 case-patients, 7 controls); chronic gastrointestinal illness (221 case-patients, 324 controls); gastrointestinal symptoms in the preceding 14 days (431); international travel in the preceding 14 days (560 case-patients, 511 controls); and being part of a household cluster of gastrointestinal illness (6 case-patients). After exclusions, 1,592 cases and 3,983 controls were available for analysis. Among controls, 2,486 (62.4%), 700 (17.6%), and 689 (17.3%) questionnaires were completed after the initial contact, first reminder, and second reminder respectively. Date of questionnaire completion was unknown or implausible for 108 controls.
Single-Variable Analysis
Habitual factors associated with increased risk were self-reported diarrheal illness in the previous 12 months; self-reported past Campylobacter enteritis; use of antimicrobial drugs, antacids and acid-suppressing medications in the previous 28 days; diabetes; puppy ownership; recent dog acquisition; chicken consumption at least once a week; red meat consumption once a week; and sharing of kitchen facilities. Eating commercially prepared chicken in the previous 5 days also was associated with increased risk (Table 1).
Habitual factors associated with decreased risk for illness were vegetarianism; regular consumption of salads, rice, and legumes; occupational exposure to sheep and horses; ownership of fish or rodents; and regular drinking of unpasteurized milk. Consumption of unpasteurized milk and dairy products, noncarbonated and carbonated bottled water, and unfiltered tap water in the previous 5 days also was associated with decreased risk.
Final Multivariable Model
In the final model, positively associated exposures were past Campylobacter enteritis (OR 2.2, 95% CI 1.3–3.6), recent use of acid-suppressing medication (OR 3.4, 95% CI 2.5–4.6), recent acquisition of a dog (OR 14.4, 95% CI 3.7–54.1), regular consumption of chicken (OR 3.7, 95% CI 2.1–6.8 for those eating chicken >5 times a week), and consumption of commercially prepared chicken only in the previous 5 days (OR 2.0, 95% CI 1.3–3.0). Regular consumption of salads, legumes, and unpasteurized milk and consumption of home-prepared chicken in the previous 5 days were associated with decreased risk (Table 2).
Chicken Consumption (Interaction Model)
Figure
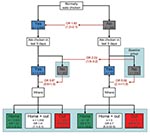
Figure. Odds ratios (ORs) and 95% confidence intervals (shown in parentheses) for Campylobacter enteritis associated with chicken consumption, England, 2005–2006. Numbers in boxes represent persons in each category; Numbers in red indicate...
Statistical evidence was strong for an interaction between regular and recent chicken consumption (LR test p = 0.0002) (Figure). Overall, persons who regularly ate chicken (at least once a week) were at greater risk for illness than those who did not (OR 1.6, 95% CI 1.2–2.0) (Figure, top). However, for persons who did not regularly eat chicken, eating it in the previous 5 days posed a 5-fold greater risk than it did for persons who did not (OR 5.0, 95% CI 2.1–11.9). We did not see this association for persons who regularly ate chicken (OR 0.8, 95% CI 0.6–1.0) (Figure, middle).
The risk associated with eating commercially prepared chicken was greater than that associated with eating home-prepared chicken. Among persons who regularly ate chicken, eating commercially prepared chicken in the previous 5 days was associated with a 4-fold increased risk (OR 4.0, 95% CI 2.8–5.8) for Campylobacter infection, much higher than the risk associated with eating home-prepared chicken (OR 1.5, 95% CI 1.1–2.1). Among those who did not regularly eat chicken, eating commercially prepared chicken was associated with a 36-fold increased risk (OR 35.7, 95% CI 3.7–344.1); however, this group was very small (Figure, bottom).
Adjusting for nonchicken-related factors had little effect on the ORs (Table 2). The p values were considerably higher, although this analysis was based on fewer persons because of missing data in some variables.
Sensitivity Analyses
Excluding late-responding case-patients had little effect on the ORs in either the final multivariable model or the interaction model. In the final multivariable model, ORs for eating chicken >1 times per week were consistently higher than in the model comprising all cases (OR 5.4, 95% CI 2.3–12.4 for eating chicken >5 times per week).
In the inverse probability-weighted final model, the OR for eating commercially prepared chicken in the previous 5 days was 1.6 (95% CI 0.98–2.62). Other results did not change. In the interaction model, the weighted model indicated stronger evidence for associations with eating home-prepared chicken (OR 1.76, 95% CI 1.22–2.29, p = 0.001) and eating home-prepared and commercially prepared chicken in the previous 5 days (OR 1.63, 95% CI 1.18–2.25, p = 0.003), compared with the unweighted results (Table 1).
Population-Attributable Fractions
Chicken-related exposures were reported by 92.5% of controls; use of acid-suppressing medications, by 6.0%; past Campylobacter enteritis, by 2.2%; and recent acquisition of a dog, by 1.6%. The percentage of cases attributable to each of these risk factors (Table 3) was as follows: chicken-related exposures, 41%; acid-suppressing medications, 10%; past Campylobacter enteritis, 3%; and recent acquisition of a dog, 1%.
Chicken consumption and use of acid-suppressing medications are major risk factors for Campylobacter enteritis in England. Chicken-related exposures accounted for 41% of adult cases, consistent with previous US and Australian studies (5,8,24). Recent use of acid-suppressing medications increased risk for illness 3-fold, similar to other studies (9), accounting for 10% of cases.
Like others (3,6–8,11), we found that commercially prepared chicken poses a greater risk than home-prepared chicken. Reasons might be greater contamination levels or inadequate cooking procedures, which could be more common in commercial establishments than in homes. However, we found only modest increases in risk for persons who ate home-prepared and commercially prepared chicken, suggesting that persons who regularly eat chicken at home frequent different types of establishments than do persons who tend to eat chicken only outside the home. We could not investigate this hypothesis further.
Several findings suggest that acquired immunity might be important. The risk for Campylobacter enteritis associated with recent chicken consumption depended on whether participants regularly ate chicken. For persons who ate chicken in the previous 5 days, the risk was considerably greater for those who did not regularly eat chicken than for those who did. Recent, but not longer-term, dog owners had higher risk for illness, whereas persons who regularly drank unpasteurized milk had decreased risk. We could not confirm participants’ immunologic status; however, these results suggest that long-term exposure to these sources of Campylobacter spp. might confer partial immunity (25). In immunologically susceptible populations, however, unpasteurized milk is a well-known cause of outbreaks of infection with Campylobacter and potentially fatal Shiga–toxin producing Escherichia coli (26). Further developments to characterize relevant correlates of immune status for Campylobacter infection are required to confirm these findings.
Despite the potential role of immunity, participants reporting previous Campylobacter enteritis, but not nonspecific enteritis, had greater risk for recent Campylobacter illness than did persons not reporting past Campylobacter enteritis. Compared with all cases, those reporting a previous episode of Campylobacter enteritis were of similar age but more likely to be female (57% vs. 49%). These persons may differ in other ways that increase risk, such as medical history or immune competence. However, this finding should be interpreted cautiously because we had no independent confirmation of self-reported Campylobacter enteritis.
Other researchers (11) have suggested that regular consumption of vegetables and legumes might protect against infection. However, eating these foods might simply be a marker for unmeasured behavior related to decreased risk.
We found no associations with any environmental variables. Environmental exposures may pose low or transient risk; temporal variation in environmental prevalence of Campylobacter spp. could make their effects difficult to detect. Previous studies in England have identified diabetes as a risk factor for Campylobacter enteritis (9); in our study, initial analyses suggested a 1.5-fold increase in illness associated with diabetes, but this effect disappeared after adjustment for other habitual factors.
We did not include persons who reported recent international travel because travel-related illness may have different risk factors. However, international travel is common among persons in England with laboratory-confirmed Campylobacter infection; 24% of all case-patients reported traveling abroad in the previous 14 days compared with 11% of controls.
Our analysis emphasizes the importance of accounting for regular dietary habits in determining risk associated with recent consumption of putatively risky foods. Moreover, selection of an appropriate baseline comparison group (in this case, persons truly unexposed to chicken consumption) is crucial to enable meaningful comparisons. In the future, distinguishing long-term and recent exposures will be important in investigating how their association influences risk. More detailed study of the risks associated with chicken prepared at home and in commercial establishments is needed. Given the limitations of case–control studies for collecting long-term exposure information, innovative studies using a variety of approaches are necessary.
In England, chicken consumption is the major recognized risk factor for Campylobacter enteritis. Understanding the differing risks from poultry sources should guide strategies to reduce risk for infection from chicken. Immunologic factors appear to be important in determining risk for Campylobacter enteritis given exposure to infection. Meaningful interpretation of Campylobacter risk factor studies requires better knowledge of population susceptibility to infection and the extent to which past exposure can induce protection. Identifying relevant immune correlates would help determine whether differences in immune status, behavior, or both are responsible for differing risks for Campylobacter enteritis between populations or population subgroups.
Dr Tam is lecturer in epidemiology at the London School of Hygiene and Tropical Medicine. His main research interests are the epidemiology of gastrointestinal infections, long-term consequences of gastrointestinal infections, and the epidemiology of dengue fever.
Acknowledgments
We thank Tracey Wood and Maria Davies for assistance with data collection in Cheshire and Merseyside and staff at the Environmental Health Departments at the respective study sites for supplying data for the study.
This study was funded by the United Kingdom Food Standards Agency (project no. B14011).
References
- Health Protection Agency. Campylobacter spp.: laboratory reports of faecal isolates reported to the Health Protection Agency Centre for Infections [cited 2008 Feb 1]. Available from http://www.hpa.org.uk/infections/topics_az/campy/data_ew.htm
- Wheeler JG, Sethi D, Cowden JM, Wall PG, Rodrigues LC, Tompkins DS, Study of infectious intestinal disease in England: rates in the community, presenting to general practice, and reported to national surveillance. The Infectious Intestinal Disease Study Executive. BMJ. 1999;318:1046–50.PubMedGoogle Scholar
- Unicomb LE, Dalton CB, Gilbert GL, Becker NG, Patel MS. Age-specific risk factors for sporadic Campylobacter infection in regional Australia. Foodborne Pathog Dis. 2008;5:79–85. DOIPubMedGoogle Scholar
- Gallay A, Bousquet V, Siret V, Prouzet-Mauleon V, Valk H, Vaillant V, Risk factors for acquiring sporadic Campylobacter infection in France: results from a national case–control study. J Infect Dis. 2008;197:1477–84. DOIPubMedGoogle Scholar
- Stafford RJ, Schluter P, Kirk M, Wilson A, Unicomb L, Ashbolt R, A multi-centre prospective case–control study of Campylobacter infection in persons aged 5 years and older in Australia. Epidemiol Infect. 2007;135:978–88. DOIPubMedGoogle Scholar
- Eberhart-Phillips J, Walker N, Garrett N, Bell D, Sinclair D, Rainger W, Campylobacteriosis in New Zealand: results of a case–control study. J Epidemiol Community Health. 1997;51:686–91. DOIPubMedGoogle Scholar
- Effler P, Ieong MC, Kimura A, Nakata M, Burr R, Cremer E, Sporadic Campylobacter jejuni infections in Hawaii: associations with prior antibiotic use and commercially prepared chicken. J Infect Dis. 2001;183:1152–5. DOIPubMedGoogle Scholar
- Friedman CR, Hoekstra RM, Samuel M, Marcus R, Bender J, Shiferaw B, Risk factors for sporadic Campylobacter infection in the United States: a case–control study in FoodNet sites. Clin Infect Dis. 2004;38(Suppl 3):S285–96. DOIPubMedGoogle Scholar
- Neal KR, Slack RC. Diabetes mellitus, anti-secretory drugs and other risk factors for Campylobacter gastro-enteritis in adults: a case–control study. Epidemiol Infect. 1997;119:307–11. DOIPubMedGoogle Scholar
- Neimann J, Engberg J, Molbak K, Wegener HC. A case–control study of risk factors for sporadic Campylobacter infections in Denmark. Epidemiol Infect. 2003;130:353–66.PubMedGoogle Scholar
- Rodrigues LC, Cowden JM, Wheeler JG, Sethi D, Wall PG, Cumberland P, The study of infectious intestinal disease in England: risk factors for cases of infectious intestinal disease with Campylobacter jejuni infection. Epidemiol Infect. 2001;127:185–93. DOIPubMedGoogle Scholar
- Ikram R, Chambers S, Mitchell P, Brieseman MA, Ikam OH. A case control study to determine risk factors for Campylobacter infection in Christchurch in the summer of 1992–3. N Z Med J. 1994;107:430–2.PubMedGoogle Scholar
- Kapperud G, Skjerve E, Bean NH, Ostroff SM, Lassen J. Risk factors for sporadic Campylobacter infections: results of a case–control study in southeastern Norway. J Clin Microbiol. 1992;30:3117–21.PubMedGoogle Scholar
- Michaud S, Menard S, Arbeit RD. Campylobacteriosis, Eastern Townships, Quebec. Emerg Infect Dis. 2004;10:1844–7.PubMedGoogle Scholar
- Studahl A, Andersson Y. Risk factors for indigenous Campylobacter infection: a Swedish case–control study. Epidemiol Infect. 2000;125:269–75. DOIPubMedGoogle Scholar
- Tenkate TD, Stafford RJ. Risk factors for Campylobacter infection in infants and young children: a matched case–control study. Epidemiol Infect. 2001;127:399–404. DOIPubMedGoogle Scholar
- Wingstrand A, Neimann J, Engberg J, Nielsen EM, Gerner-Smidt P, Wegener HC, Fresh chicken as main risk factor for campylobacteriosis, Denmark. Emerg Infect Dis. 2006;12:280–5.PubMedGoogle Scholar
- Danis K, Di Renzi M, O’Neill W, Smyth B, McKeown P, Foley B, Risk factors for sporadic Campylobacter infection: an all-Ireland case–control study. Euro Surveill. 2009;14:pii=19123.
- Adak GK, Cowden JM, Nicholas S, Evans HS. The Public Health Laboratory Service national case–control study of primary indigenous sporadic cases of Campylobacter infection. Epidemiol Infect. 1995;115:15–22. DOIPubMedGoogle Scholar
- Evans MR, Ribeiro CD, Salmon RL. Hazards of healthy living: bottled water and salad vegetables as risk factors for Campylobacter infection. Emerg Infect Dis. 2003;9:1219–25.PubMedGoogle Scholar
- Infectious Intestinal Disease Study Team. A report of the study of infectious intestinal disease in England. London: The Stationery Office; 2000.
- Cole SR, Hernan MA, Robins JM, Anastos K, Chmiel J, Detels R, Effect of highly active antiretroviral therapy on time to acquired immunodeficiency syndrome or death using marginal structural models. Am J Epidemiol. 2003;158:687–94. DOIPubMedGoogle Scholar
- The English indices of deprivation 2004: summary (revised) [cited 2009 Jun 30] Available from http://www.rbkc.gov.uk/kcpartnership/General/pc_indices_deprivation.pdf
- Stafford RJ, Schluter PJ, Wilson AJ, Kirk MD, Hall G, Unicomb L. Population-attributable risk estimates for risk factors associated with Campylobacter infection, Australia. Emerg Infect Dis. 2008;14:895–901. DOIPubMedGoogle Scholar
- Blaser MJ, Sazie E, Williams LP Jr. The influence of immunity on raw milk–associated Campylobacter infection. JAMA. 1987;257:43–6. DOIPubMedGoogle Scholar
- Frost JA, Gillespie IA, O’Brien SJ. Public health implications of Campylobacter outbreaks in England and Wales, 1995–9: epidemiological and microbiological investigations. Epidemiol Infect. 2002;128:111–8. DOIPubMedGoogle Scholar
Figure
Tables
Cite This Article1The Campylobacter Case–Control Study Group comprises the following: Sarah J. O’Brien (Manchester University); Clarence C. Tam, Craig D. Higgins, Laura C. Rodrigues, and Brendan W. Wren (London School of Hygiene and Tropical Medicine); Keith R. Neal (University of Nottingham); Bob Owen and Judith Richardson (Health Protection Agency Centre for Infections); Bharat C. Patel (Health Protection Agency Collaborating Centre, North Middlesex Hospital); Peter Sheridan (North East and Central London HPU); John Curnow (Cheshire and Merseyside HPU); Ken Lamden (Cumbria and Lancashire HPU); and Sally Millership (Essex HPU).
Table of Contents – Volume 15, Number 9—September 2009
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Clarence C. Tam, Infectious Disease Epidemiology Unit, Department of Epidemiology and Population Health, London School of Hygiene and Tropical Medicine, Keppel Street, London WC1E 7HT, UK;
Top