Volume 25, Number 10—October 2019
Research
Sensitive and Specific Detection of Low-Level Antibody Responses in Mild Middle East Respiratory Syndrome Coronavirus Infections
Nisreen M.A. Okba, V. Stalin Raj, Ivy Widjaja, Corine H. GeurtsvanKessel, Erwin de Bruin, Felicity D. Chandler, Wan Beom Park, Nam-Joong Kim, Elmoubasher A.B.A. Farag, Mohammed Al-Hajri, Berend-Jan Bosch, Myoung-don Oh, Marion P.G. Koopmans, Chantal B.E.M. Reusken, and Bart L. Haagmans
Figure 3
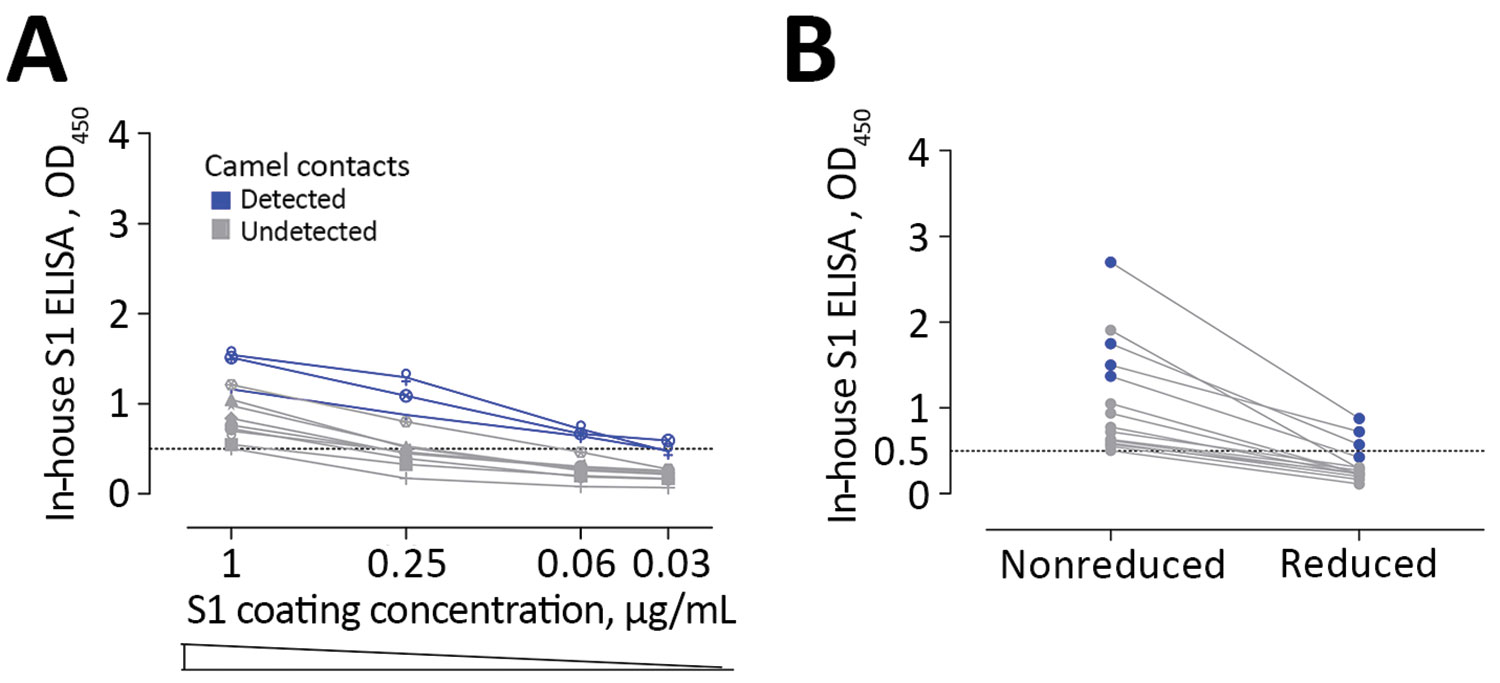
Figure 3. Low sensitivity of commercial S1 ELISA shown as the effect of lowering coating antigen concentration (A) or antigen denaturation (B) on the sensitivity of antibody detection among Middle East respiratory syndrome coronavirus–infected persons with camel contact. All samples were seropositive by in-house S1 ELISA and microarray. Dark blue indicates those that tested seropositive by commercial S1 ELISA.
Page created: September 17, 2019
Page updated: September 17, 2019
Page reviewed: September 17, 2019
The conclusions, findings, and opinions expressed by authors contributing to this journal do not necessarily reflect the official position of the U.S. Department of Health and Human Services, the Public Health Service, the Centers for Disease Control and Prevention, or the authors' affiliated institutions. Use of trade names is for identification only and does not imply endorsement by any of the groups named above.