Volume 28, Number 6—June 2022
Research
Risk Prediction Score for Pediatric Patients with Suspected Ebola Virus Disease
Alicia E. Genisca1 , Tzu-Chun Chu1, Lawrence Huang, Monique Gainey, Moyinoluwa Adeniji, Eta N. Mbong, Stephen B. Kennedy, Razia Laghari, Fiston Nganga, Rigo F. Muhayangabo, Himanshu Vaishnav, Shiromi M. Perera, Andrés Colubri2, Adam C. Levine2, and Ian C. Michelow23
, Tzu-Chun Chu1, Lawrence Huang, Monique Gainey, Moyinoluwa Adeniji, Eta N. Mbong, Stephen B. Kennedy, Razia Laghari, Fiston Nganga, Rigo F. Muhayangabo, Himanshu Vaishnav, Shiromi M. Perera, Andrés Colubri2, Adam C. Levine2, and Ian C. Michelow23
Figure 3
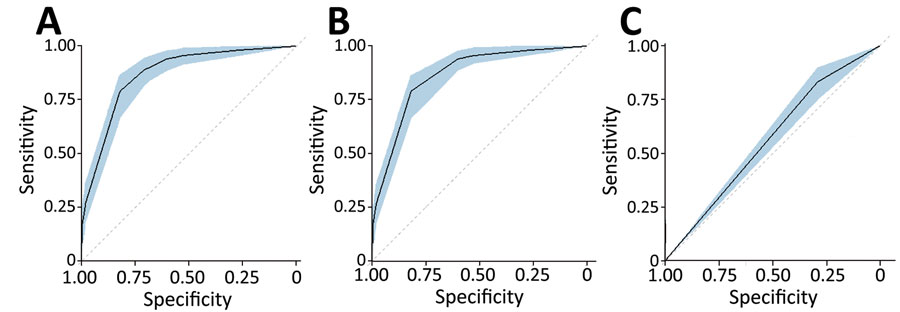
Figure 3. Comparison of strength of discrimination using areas under the curve for study of risk prediction score for pediatric patients with suspected Ebola virus disease in West Africa. A) Ebola diagnostic model; B) Pediatric Ebola Risk Score; C) World Health Organization criteria. The shaded blue regions within each of the panels represent the confidence bands for the areas under the curve.
1These authors contributed equally to this article.
2These authors contributed equally to this article.
3Current affiliation: Pediatric Infectious Diseases & Immunology, Connecticut Children’s Medical Center, Hartford, Connecticut, USA.
Page created: April 11, 2022
Page updated: May 22, 2022
Page reviewed: May 22, 2022
The conclusions, findings, and opinions expressed by authors contributing to this journal do not necessarily reflect the official position of the U.S. Department of Health and Human Services, the Public Health Service, the Centers for Disease Control and Prevention, or the authors' affiliated institutions. Use of trade names is for identification only and does not imply endorsement by any of the groups named above.