Volume 30, Number 12—December 2024
Online Report
Operational Risk Assessment Tool for Evaluating Leishmania infantum Introduction and Establishment in the United States through Dog Importation1
Cite This Article
Citation for Media
Abstract
International pet travel and commercial operations have increased animal disease importation risks, including for Leishmania infantum, a deadly parasite of humans and domestic dogs. Collaborating as an interdisciplinary working group, we developed an operational tool for veterinary and public health practitioners to assess and manage L. infantum risk in dogs imported to the United States. Overall risk varies by dog, human, and geographic factors but could be high without proper controls. We determined dog risk management strategies should include application of sand fly insecticides and repellents, sterilization, and treatment. US public health authorities can use a One Health approach to manage L. infantum importation risks via infected dogs.
International pet travel and importation of breeding and rescue animals have increased substantially, spreading diseases beyond established geographic distributions (1–3). The Centers for Disease Control and Prevention (CDC) estimates 1 million dogs cross US borders annually (4). Despite cooperation among federal agencies, <0.3% of dogs receive animal import certifications, and most do not receive adequate infectious disease screening before entering the United States (2,4,5).
Unregulated dog importation into the United States from leishmania-endemic countries could continue to introduce Leishmania infantum, one of the world’s deadliest tropical parasites (6). L. infantum is a protozoal parasite that causes zoonotic visceral leishmaniasis (ZVL) in humans and canine leishmaniosis (CanL) in dogs. Dogs are the primary reservoir hosts in endemic areas, which include southern Europe, North Africa, the Middle East, Central Asia, China, and South and Central America (7). Annually, an estimated 10,000–18,000 ZVL cases are reported globally, and disease is usually fatal without treatment (8). Domestically acquired human ZVL cases have not been identified within the United States, but CanL has been found in US hunting dogs across 60 kennels and 28 states since the early 2000s (9,10). However, the parasite is spreading because of globalization and climate change (11–13). Over the past 20 years, dog movements resulted in >1,400 nonautochthonous canine Leishmania spp. infections in multiple countries (11). Almost all L. infantum–positive nonhunting dogs in the United States have history of travel to L. infantum–endemic areas (14).
L. infantum parasites are prevalent among hunting dogs in several US states, but few states have formal disease surveillance and control programs (15). The number of L. infantum–infected dogs imported into the United States is unknown, as is the risk importation poses for establishing autochthonous ZVL and further spread of CanL among US nonhunting dogs. We devised an operational risk assessment tool (ORAT) to address the probability of importing L. infantum–infected dogs into the United States from endemic areas, the probability of vectored transmission via sand flies among US dogs, and potential impacts of autochthonous L. infantum parasite transmission on canine and human health. The tool provides public and animal health officials with a risk assessment framework and evidence-based mitigation recommendations when importing potentially infected dogs from L. infantum–endemic countries.
An interdisciplinary working group whose members have backgrounds in veterinary epidemiology, infectious diseases, public health, vector ecology, and risk sciences, developed this ORAT by using established qualitative risk assessment frameworks (16–21). Risk assessment occurs in 3 phases. First, the hazard is identified along with key assumptions needed for characterizing the hazard and risks that the hazard will occur. Next, necessary steps for the hazard to occur are defined as the entry and exposure assessments, and the probability of each step occurring are characterized into qualitative risk categories, such as very low, low, moderate, and high. Finally, the consequence is assessed, and a final risk is determined on the basis of probability and impacts.
Figure 1

Figure 1. Scenario tree used to develop an operational risk assessment tool for evaluating Leishmania infantum introduction and establishment in the United States through dog importation. SFPs, sand fly preventatives.
Figure 2

Figure 2. Probability and impact categories for an operational risk assessment tool for evaluating Leishmania infantumintroduction and establishment in the United States through dog importation. Modified from Food and Agriculture...
Figure 3

Figure 3. Uncertainty categories for an operational risk assessment tool for evaluating Leishmania infantumintroduction and establishment in the United States through dog importation. Modified from Food and Agriculture Organization of...
In this ORAT, the entry assessment considers the probability of importing L. infantum–infected dogs into the United States, the exposure assessment estimates the potential for vector transmission by domestic sand fly species, and the consequence assessment considers the impact of autochthonous L. infantum transmission on dog and human health (Figure 1). This risk assessment used expert opinion combined with a review of current available evidence at each phase. We describe the rationale for each probability and the uncertainty of the evidence (Figures 2, 3).
Hazard Identification
Figure 4

Figure 4. Parasite lifecycle used to develop an operational risk assessment tool for evaluating Leishmania infantumintroduction and establishment in the United States through dog importation. Reproduced from Esche et al....
The biologic hazard is L. infantum, which is primarily transmitted by female sand flies (genus Phlebotomus or Lutzomyia), but vertical and horizontal transmission have been increasingly documented in dogs (10,22–27). L. infantum parasites evade immune recognition and multiply within macrophages in major organs, such as the skin, liver, spleen, and bone marrow (28,29) (Figure 4). Inflammatory cytokine and immunoglobulin production results in nonspecific clinical signs such as fever, weight loss, and organomegaly. Dogs develop prominent dermatological lesions and glomerulonephritis, which greatly reduces prognosis in advanced stages (28,30). Immunocompromised persons are at greatest risk for disease progression, particularly persons with HIV (8), pregnant women (31), children (8), and intravenous drug users (32). Poor nutrition, co-infections, and stress may exacerbate CanL and ZVL disease progression (29,33).
L. infantum–infected dogs are highly prevalent in endemic areas, are difficult to identify and treat, and pose disease transmission risks to other animals and humans. L. infantum parasites are prevalent among hunting dogs in several US states but otherwise are not endemic. In the United States, L. infantum parasites are passed from infected dams to pups without apparent vector transmission, making vertical transmission the dominant mode of disease spread (10,23,34). Despite experimental studies confirming parasite transmission from sand flies fed on infected hunting dogs (35), no evidence of vectored L. infantum transmission among US dogs or humans has been reported (9,10,35). The United States has >14 sand fly species, and 3 are known vectors of Leishmania parasites: Lutzomyia anthophora, Lu. diabolica, and Lu. shannoni (36–38). Lu. anthophora and Lu. diabolica sand flies are known vectors of L. mexicana parasites (37,39–41) but not of other Leishmania spp. in the United States. Studies of Lu. shannoni sand flies raise concern that it could be a permissive vector for L. infantum (35,42).
US importation of asymptomatic, infected dogs remains a likely route of Leishmania parasite entry (14). For this risk assessment tool, we considered L. infantum a substantial hazard in domestic dogs imported from endemic areas into the United States.
Key Assumptions Used in ORAT Development
Key assumptions we used for developing the ORAT were reservoirs, vectors, and preventive measures. For reservoirs, we considered dogs imported into the United States to represent the general US dog population that are equally susceptible to L. infantum infection and are equally infectious to sand flies (i.e., not super spreaders) (43,44). We considered vectors to include Lu. shannoni sand flies, which could act as permissive vectors for L. infantum transmission among dogs. For preventive measures, we considered sand fly preventatives to include insecticidal and repellent collars, sprays, and topicals experimentally shown to reduce sand fly feeding and lifespans. For this ORAT, we assumed that US sand flies are susceptible to commercially available SFPs and products are correctly applied on dogs according to manufacturer’s guidelines.
Entry Assessment
Figure 5

Figure 5. Probability scale used to develop an operational risk assessment tool for evaluating Leishmania infantumintroduction and establishment in the United States through dog importation. *Negative serologic titers are typically...
The entry assessment describes biologic pathways needed for importation of an infected dog to introduce L. infantum parasites into the United States (Figure 5) and estimates the probability of that process occurring (19). Entry assessment rationale considers that prevalence estimates of infected dogs in endemic countries range from 3% to 24% but can exceed 70% in highly endemic areas (7,46–48). Officials tasked with assessing risk (risk assessors) posed by an imported dog should consider the dog’s country of origin and that country’s endemicity status (19) (Appendix), in addition to individual factors, such as time spent in endemic areas, SFP use, and the dog’s occupation, to determine the dog’s infection probability during the entry assessment.
Dogs traveling to L. infantum–endemic areas for <3 weeks are at low risk (<1%) for infection, particularly if prophylactically treated with SFPs (6,49–50; Appendix reference 51). Infection risk increases with time spent in endemic areas, particularly for dogs outdoors during sand fly season (7). L. infantum vaccines available in Europe and Brazil have varying levels of protection but may reduce infection rates in healthy seronegative dogs (Appendix reference 52).
Most L. infantum–infected dogs are asymptomatic, creating challenges assessing importation risks in healthy, traveling pets. Serologic diagnostic tests such as indirect fluorescent antibody tests (IFAT) and ELISA are widely used but may cross-react with antibodies to Trypanosoma cruzi parasites (Appendix reference 53). Quantitative L. infantum serologic titers >1:320 are often associated with high parasitism and CanL in dogs with clinically suspected infections (Appendix reference 54). Low L. infantum titers indicate parasite exposure but not necessarily active infection (33; Appendix reference 55). Risk assessors should carefully weigh the dog’s clinical signs, clinicopathologic abnormalities, and serologic status during entry assessment.
Properly applied SFPs decrease sand fly feeding and survival, drastically reducing risk for L. infantum transmission in both endemic and nonendemic areas (Appendix references 51,56–61). Many pyrethroid topical products have 90% insecticidal and repellent efficacy of <4 weeks duration post application (Appendix reference 56). Dogs treated with deltamethrin or flumethrin collars or fluralaner oral insecticides were protected from sand fly bites for >5 months (Appendix reference 61–65). Newer generation insecticides, such as spinosad and isoxazolines, may be effective for preventing sand fly bites but lack clinical evidence supporting their use to prevent CanL (Appendix references 56,66,67). Natural compounds (e.g., neem oil and citronella) have limited insecticidal and repellency efficacy and are not recommended as SFPs for dogs (Appendix references 68–70).
A dog’s lifestyle or occupation greatly influences its risk of acquiring infectious diseases (Appendix reference 71). Stray and shelter dogs in endemic countries are exposed to many zoonotic parasites, including L. infantum, and pose an elevated infection risk compared with companion dogs (48; Appendix references 72,73). Working and companion dogs with frequent outdoor exposure are at increased risk for sand fly bites (13; Appendix references 71,74–76). Many governmental agencies provide SFPs for working dogs to reduce sand fly exposure, greatly reducing L. infantum infection rates in that cohort (Appendix references 71,74,77).
Entry Assessment Uncertainty Level—Low
Sufficient studies are available to characterize the entry assessment, with few discrepancies. On average, dogs develop L. infantum antibodies 5 months after infection (Appendix reference 54). Generally, IFAT, the diagnostic test used most often in the veterinary field (Appendix reference 78), has a high sensitivity (≈90%) in symptomatic and lower sensitivity (<40%) in asymptomatic dogs in endemic areas (Appendix reference 79). That sensitivity and the prolonged incubation period limit the utility of testing dogs for L. infantum infection before importation. A negative serologic result does not rule out subclinical infections in dogs (33,45); monitoring for CanL after import should continue regardless of serologic status before entry.
SFP use in L. infantum–endemic areas effectively reduces CanL incidence, particularly in working, stray, and shelter dogs. However, studies of different commercial formulations show variations in duration of protection against sand fly bites (Appendix references 65,80). Furthermore, SFPs are never 100% effective and often show substantial decreases in insecticidal activity before product reapplication. For instance, after application, many monthly ectoparasiticidal topicals lose 75% of sand fly insecticidal activity by 21 days (Appendix references 81,82). Appropriate SFP use is also difficult to monitor because it is the responsibility of the dog’s owner or caretaker.
Vaccines used in Brazil and Europe are likely to prevent clinical disease progression, but reports conflict as to whether vaccines prevent CanL infections in endemic areas (6; Appendix references 52,83,84). Further studies are needed before vaccinated dogs can be considered low risk for introducing L. infantum (Appendix reference 83).
Exposure Assessment
Figure 6

Figure 6. Probability of vectored transmission scale used to develop an operational risk assessment tool for evaluating Leishmania infantumintroduction and establishment in the United States through dog importation. SFPs, sand...
The exposure assessment describes biologic pathways required for release of L. infantum parasites from an infected imported dog and subsequent exposure of humans and other animals in the United States and assesses the likelihood of occurrence (19) (Figure 6). The exposure assessment rationale considers that not all sand fly species are competent vectors (i.e., susceptible to infection with L. infantum parasites and capable of transmitting to vertebrate hosts) of Leishmania spp. (Appendix reference 85), but many are considered permissive vectors, whereby they support development of Old and New World Leishmania parasites but do not further transmit parasites (Appendix references 86,87). Vector competence and permissiveness are laboratory-defined terms. Few studies have assessed L. infantum infection rates of US sand flies, but experimental studies have shown Lu. shannoni sand flies support parasite development after feeding on infected dogs and hamsters, making it a permissive vector (35,42).
Lu. shannoni sand flies are widely dispersed across the United States and reported from >17 states (36; Appendix references 88–93). Within its range, Lu. shannoni sand fly occurrence is subject to local environmental factors, including precipitation, temperature, habitat availability, and suitable hosts (Appendix reference 94). The flies feed primarily on mammals, including rodents, livestock, dogs, and deer, and will readily feed on humans (36; Appendix references 92,95).
Figure 7
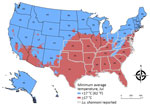
Figure 7. Minimum average July temperatures used to develop an operational risk assessment tool for evaluating Leishmania infantumintroduction and establishment in the United States through dog importation. Map shows areas...
Sand flies develop, feed, and thrive at 20°C–28°C (68°F–82°F) (Appendix references 96–98), and 17°C (62°F) is considered the minimum sand fly survival temperature (Appendix reference 56). We devised a risk map by using estimates of potential US sand fly distribution overlayed with average minimum temperatures during peak sand fly season (Figure 7), similar to the L. infantum risk map from Europe (Appendix reference 56). The map does not include humidity, wind, or rain estimates but assesses geographic areas with temperatures above and below 17°C in July, historically the warmest month of the year, to conservatively predict sand fly activity. The map demonstrates states at higher risk for L. infantum vector-borne transmission due to reported Lu. shannoni sand fly activity (Figure 7, outlined in white dotted lines).
Treatment of CanL in dogs rarely produces a parasitic cure but reduces clinical signs, parasite burden, and risk for transmission to sand flies for >4 months (Appendix references 70,80,100–104). However, many dogs will relapse and become infectious to sand flies within a year posttreatment (Appendix references 101,105,106). Second- and third-line therapeutics, such as metronidazole, marbofloxacin, and azole antifungals, improve clinical signs associated with CanL but have not been evaluated for alteration of parasitemia in dogs and did not reduce hepatic parasite loads in mice (Appendix references 107–109).
Exposure Assessment Uncertainty Level—High
Climate change has undoubtedly altered sand fly species’ geographic distribution and seasonality, likely increasing the risk for new L. infantum infections (Appendix references 86,88,110). However, the potential magnitude of sand fly habitat expansion within the United States is unknown. Whether US sand fly species, particularly Lu. shannoni, can transmit L. infantum parasites to uninfected animals or humans in natural settings is also unknown (42; Appendix reference 111). Additional studies are needed to confirm Lu. shannoni vector competence in natural settings.
Despite clinical improvement and reduced infectiousness to sand flies after therapy, treated dogs may still harbor viable parasites that sand flies could ingest (Appendix references 112–115). Not all chemotherapeutic drugs substantially reduce parasitic loads. Chemotherapy may be less effective at reducing parasitic loads in drug-resistant strains, which are reported for meglumine antimoniate and allopurinol in some areas (Appendix references 116,117). Additional studies in dogs are needed to establish whether azole antifungal drugs further reduce dog infectivity to sand flies (Appendix reference 118).
Figure 8
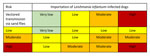
Figure 8. Combined probability matrix for entry and exposure assessments developed from an operational risk assessment tool for evaluating Leishmania infantumintroduction and establishment in the United States through dog importation....
Results from numerous studies have identified positive associations between the severity of an infected dog’s clinical and laboratory findings and its infectiousness to sand flies (Appendix references 119–123). However, clinical scores used to define severity in those studies were highly variable and might not have accounted for all clinicopathologic abnormalities or skin parasite burden, making comparison of patient infectiousness across studies challenging (Appendix reference 124). Results from more recent studies have established skin parasitic burden as most predictive of transmission and demonstrated that mildly affected dogs were more infectious to sand flies than were severely affected dogs (44). When working through the ORAT, the entry and exposure probabilities can be combined in a combination probability matrix that determines conditional probability estimates of L. infantum parasite importation via infected dogs, followed by vectorborne transmission in the United States (Figure 8).
Consequence Assessment
Figure 9

Figure 9. Scenarios and possible impact of autochthonous transmission on dog and human health used to develop an operational risk assessment tool for evaluating Leishmania infantumintroduction and establishment in the...
The consequence assessment considers biologic (health) consequences for further establishment of L. infantum in the general dog population and its impact on human and dog health (19). Health consequences are expected to vary depending on immune status, treatment response of infected humans and dogs, and the broader public health impact of autochthonous infections. Immunosuppressed persons are at greatest risk for major adverse consequences (Appendix reference 125). Although uncommon, veterinary and research personnel may be infected while working with infected animals or biologic samples (Appendix references 126). Other biologic considerations include illness and death, transmissibility, adverse treatment responses, and prognosis. We summarized consequence assessments for selected scenarios of L. infantum introduction through dog importation into the United States (Figure 9), which we adapted from the World Organisation for Animal Health (19).
Most L. infantum parasitic infections in dogs (85%–90%) and humans (95%–97%) are asymptomatic (33; Appendix references 127,128). Reports suggest that <25% of exposed dogs in endemic areas mount effective immune responses and might resolve infection, even without treatment (Appendix references 129,130). Asymptomatic infected dogs on appropriate SFPs are unlikely to create major public health risks for immunocompetent persons nearby (29,33).
CanL is rarely diagnosed in the United States, and veterinary professionals’ unfamiliarity could lead to delayed clinical suspicion and diagnosis. Once diagnosed, prognosis depends on the dog’s clinical stage and renal function when therapy is initiated (Appendix reference 130). Among symptomatic nonproteinuric dogs treated for CanL, 75% survive >4 years, but in dogs with proteinuria, an indicator of impaired renal function, mean survival time is reduced to ≈2 years (Appendix references 130,131). Although dogs never reach parasitic cure, clinical signs improve rapidly after therapy, and prognosis is favorable with frequent veterinary monitoring (Appendix references 104,113,130,132). Treated dogs are much less infectious for months after treatment, reducing public health risks (33; Appendix references 104,133).
Many medical professionals are unaware of risk factors and clinical signs suggestive of ZVL (15), and underreporting is likely extensive, even in areas where the disease is endemic (Appendix reference 134). Delayed diagnosis and therapy can negatively impact health outcomes and increase vectorborne transmission in vulnerable populations (15; Appendix references 135,136). Asymptomatic humans can transmit L. infantum parasites via blood transfusions, organ transplants, and sand fly bites but to a lesser extent than for immunocompromised or symptomatic persons (Appendix references 137,138).
ZVL in humans is life-threatening if not appropriately treated. ZVL is especially problematic in vulnerable populations and can persist for decades after treatment (8). Persons concurrently infected with HIV generally have suboptimal clinical responses to leishmania treatment and are more likely to suffer posttreatment infection relapses (12; Appendix reference 125). Treated immunocompetent humans often attain nonsterile cure and uncommonly develop disease after infection (29,33; Appendix reference 125).
The US Food and Drug Administration (FDA) approved 2 medications for treating ZVL in humans, intravenous liposomal amphotericin B and oral miltefosine; no approved therapies are available for treating CanL in dogs. Besides allopurinol, access to leishmania treatment drugs for extralabel veterinary use is limited because of financial costs and availability within the United States.
Beyond biologic considerations, other factors need to be considered in a consequence assessment. Environmental consequences include potential L. infantum establishment in wildlife reservoirs and vectors, and environmental degradation from residual insecticides. Economic considerations include surveillance, diagnostic methods, treatment, and monitoring of dog and human cases, and preventative costs for SFPs on infected and susceptible dogs. Quantitative analysis of economic and environmental consequences of L. infantum infection is beyond the scope of this risk assessment and future research could elaborate on the impacts of establishment and spread of L. infantum parasites in the United States. However, expenses would result from detection of additional human and animal cases, treatment for infected persons, and vector control to prevent further spread. Because no licensed vaccine is approved in the United States, control efforts would primarily focus on treating infectious dogs and enforcing strict lifelong use of dog SFPs (Appendix references 139,140).
Consequence Assessment Uncertainty Level—Low
Sufficient studies characterize health consequences of establishment of autochthonous vectorborne transmission of ZVL and CanL in the United States. L. infantum parasites infect cats, rodents, and numerous other animals, but the impact of those animals on disease transmission in endemic areas is unknown (Appendix references 119,141–143). Other natural L. infantum reservoirs and their role in transmission cycles need investigation (Appendix references 137,142,144).
Final Risk Estimation Matrix
Figure 10
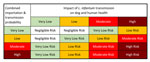
Figure 10. Final risk estimation matrix from an operational risk assessment tool for evaluating Leishmania infantumintroduction and establishment in the United States through dog importation. Modified from Biosecurity Import Risk...
A final risk estimation matrix (Figure 10) combines the probabilities of importation and vectorborne transmission (Figure 8) with the outputs of the consequence assessment. The resulting matrix enables risk assessors to evaluate the overall risk for introduction and establishment of L. infantum parasites in the United States through dog importation. Once the overall risk is determined, stakeholders can devise and employ strategies to mitigate the resulting risk.
Risk Management
Risk management strategies include those that prevent L. infantum transmission by sand fly bites, between dogs, and from dogs to humans. SFPs should be applied throughout periods of sand fly activity to prevent sand fly bites. Both topical formulations containing permethrin, imidacloprid, indoxacarb, fipronil, or combinations of those drugs, and collars impregnated with deltamethrin or flumethrin/imidacloprid combination prevent sand fly bites and are available in the United States (Appendix reference 70). Topical formulations require reapplication every 3–4 weeks and should be applied >2 days before potential exposure (6). Insecticide-impregnated collars can protect for 8–12 months and should be applied >1–2 weeks before potential exposure (6; Appendix reference 70). Infected dogs residing in or traveling to areas in the United States with potential permissible sand fly vectors should have appropriate SFPs applied according to product label directions, regardless of treatment status (Appendix reference 115). In some areas, that process might mean continual, year-round SFP use.
Dogs potentially infected with L. infantum should be excluded from breeding and blood donation activities until tested by quantitative serology 6 months after arrival in the United States and, if positive, permanently restricted from those activities (6; Appendix reference 145). Because horizontal transmission risks between dogs are possible (26,27; Appendix references 146,147), contact between potentially infected dogs and healthy seronegative dogs should be limited until quantitative serology results are available.
Vaccination for leishmaniosis can interfere with serologic testing (Appendix reference 148), but vaccination status should not preclude SFP use or testing and subsequent exclusion of seropositive dogs from breeding or blood donation. Needlesticks and open wound contamination could result in zoonotic L. infantum transmission to humans. Veterinary staff should wear gloves and exercise caution when handling infected animals to prevent accidental exposures. Immunocompromised persons should take extra precautions when handling infected animals, for example by covering open wounds and washing hands immediately after contact. Persons with zoonotic disease exposures should consult their healthcare providers. Providers can consult CDC’s Parasitic Diseases Branch (404-718-4745 or
Canine Leishmaniosis ORAT
The ORAT lays out the 5-step risk assessment process for importing potentially infected dogs from L. infantum–endemic countries (Appendix). First, assessors should determine the probability of importing an infected dog by considering the dog’s country of origin, how long the dog was in the country of origin and its lifestyle there, whether the dog was maintained on SFPs, and the results of diagnostic testing. Second, assessors should determine the probability of vectorborne transmission in the region of the United States where the dog is going, and whether sand flies are present and are competent vectors. Third, assessors should determine the combined probability of events from steps 1 and 2, using the combined probability table. Fourth, assessors should determine the impact on individual canine and human health, considering both horizontal and vertical transmission among dogs as well as iatrogenic and vectorborne transmission in both dogs and humans. Finally, assessors should determine the final risk estimate using the combined risk estimate table. We provide case studies that demonstrate the application of the ORAT and examples of appropriate risk mitigation strategies (Appendix).
L. infantum parasites are a major hazard in dogs imported from endemic areas into the United States. Risks vary depending on factors specific to the dog and to geographic and human factors. Dog-specific factors include prevalence of leishmaniosis in the originating country, in-country SFP use to prevent sand fly bites, serologic and clinical status, and the dog’s occupation or lifestyle. Geographic factors include presence of the potentially permissive sand fly vector species, Lu. shannoni. Human factors include owner compliance with recommendations regarding SFP use and excluding seropositive dogs from breeding. US domestic L. infantum transmission would incur substantial healthcare costs, surveillance, and control efforts. The L. infantum ORAT provides public health and animal health officials with a framework to comprehensively assess risks posed by imported dogs and recommends mitigation measures to prevent endemic L. infantum transmission and establishment in the United States.
Dr. Marquez is a US Army public health veterinarian who completed this work during his post-doctoral fellowship at Johns Hopkins University, Baltimore, Maryland USA. His primary research interests include foodborne and zoonotic diseases that affect military service members and their families. Dr. Straily is a veterinary epidemiologist in the Parasitic Diseases Branch, Division of Parasitic Diseases and Malaria, National Center for Emerging and Zoonotic Infectious Diseases, at the US Centers for Disease Control and Prevention. Her research interests primarily focus on foodborne parasitic diseases, soil transmitted helminths, schistosomiasis, and parasitic zoonoses.
References
- Wright I, Jongejan F, Marcondes M, Peregrine A, Baneth G, Bourdeau P, et al. Parasites and vector-borne diseases disseminated by rehomed dogs. Parasit Vectors. 2020;13:546. DOIPubMedGoogle Scholar
- McQuiston JH, Wilson T, Harris S, Bacon RM, Shapiro S, Trevino I, et al. Importation of dogs into the United States: risks from rabies and other zoonotic diseases. Zoonoses Public Health. 2008;55:421–6. DOIPubMedGoogle Scholar
- Wright I, Whitfield V, Hanaghan R, Upjohn M, Boyden P. Analysis of exotic pathogens found in a large group of imported dogs following an animal welfare investigation. Vet Rec. 2023;193:
e2996 . DOIPubMedGoogle Scholar - Centers for Disease Control and Prevention. Guidance regarding agency interpretation of “rabies-free” as it relates to the importation of dogs into the United States. Federal Register. 2019 Jan 31 [cited 2023 May 22]. https://www.federalregister.gov/d/2019-00506
- United States Department of Agriculture. Report on the importation of live dogs into the United States. 2019 Jun 25 [cited 2023 May 22]. http://www.naiaonline.org/uploads/WhitePapers/USDA_DogImportReport6-25-2019.pdf
- Herricks JR, Hotez PJ, Wanga V, Coffeng LE, Haagsma JA, Basáñez MG, et al. The global burden of disease study 2013: What does it mean for the NTDs? PLoS Negl Trop Dis. 2017;11:
e0005424 . DOIPubMedGoogle Scholar - Vilas-Boas DF, Nakasone EKN, Gonçalves AAM, Lair DF, Oliveira DS, Pereira DFS, et al. Global distribution of canine visceral leishmaniasis and the role of the dog in the epidemiology of the disease. Pathogens. 2024;13:455. DOIPubMedGoogle Scholar
- Duprey ZH, Steurer FJ, Rooney JA, Kirchhoff LV, Jackson JE, Rowton ED, et al. Canine visceral leishmaniasis, United States and Canada, 2000-2003. Emerg Infect Dis. 2006;12:440–6. DOIPubMedGoogle Scholar
- Toepp AJ, Schaut RG, Scott BD, Mathur D, Berens AJ, Petersen CA. Leishmania incidence and prevalence in U.S. hunting hounds maintained via vertical transmission. Vet Parasitol Reg Stud Reports. 2017;10:75–81. DOIPubMedGoogle Scholar
- Bruhn FRP, Morais MHF, Cardoso DL, Bruhn NCP, Ferreira F, Rocha CMBMD. Spatial and temporal relationships between human and canine visceral leishmaniases in Belo Horizonte, Minas Gerais, 2006-2013. Parasit Vectors. 2018;11:372. DOIPubMedGoogle Scholar
- World Health Organization. Leishmaniasis. 2023 Jan 12 [cited 2023 May 22]. https://www.who.int/en/news-room/fact-sheets/detail/leishmaniasis
- Martín-Sánchez J, Morales-Yuste M, Acedo-Sánchez C, Barón S, Díaz V, Morillas-Márquez F. Canine leishmaniasis in southeastern Spain. Emerg Infect Dis. 2009;15:795–8. DOIPubMedGoogle Scholar
- Gin TE, Lashnits E, Wilson JM, Breitschwerdt EB, Qurollo B. Demographics and travel history of imported and autochthonous cases of leishmaniosis in dogs in the United States and Canada, 2006 to 2019. J Vet Intern Med. 2021;35:954–64. DOIPubMedGoogle Scholar
- Curtin JM, Aronson NE. Leishmaniasis in the United States: emerging issues in a region of low endemicity. Microorganisms. 2021;9:578. DOIPubMedGoogle Scholar
- European Centre for Disease Prevention and Control. Operational tool on rapid risk assessment methodology. 2019 Mar 14 [cited 2023 May 22] https://www.ecdc.europa.eu/sites/default/files/documents/operational-tool-rapid-risk-assessment-methodolgy-ecdc-2019.pdf
- Wieland B, Dhollander S, Salman M, Koenen F. Qualitative risk assessment in a data-scarce environment: a model to assess the impact of control measures on spread of African Swine Fever. Prev Vet Med. 2011;99:4–14. DOIPubMedGoogle Scholar
- World Health Organization, Food and Agriculture Organization of the United Nations, and World Organisation for Animal Health. Joint risk assessment operational tool (JRA OT): an operational tool of the tripartite zoonoses guide. 2021 Mar 9 [cited 2023 May 22]. https://www.who.int/publications/i/item/9789240015142
- World Organisation for Animal Health. Handbook on import risk analysis for animals and animal products, 2nd edition. Paris: The Organisation; 2010.
- Food and Agriculture Organization of the United Nations. Technical guidelines on rapid risk assessment for animal health threats. FAO animal production and health guidelines no. 24. Rome: The Organization; 2021.
- Department of Agriculture and Water Resources. Biosecurity import risk analysis guidelines, 2016: managing biosecurity risks for imports into Australia. Canberra: Department of Agriculture and Water Resources; 2016.
- McKenna M, Attipa C, Tasker S, Augusto M. Leishmaniosis in a dog with no travel history outside of the UK. Vet Rec. 2019;184:441. DOIPubMedGoogle Scholar
- Toepp AJ, Bennett C, Scott B, Senesac R, Oleson JJ, Petersen CA. Maternal Leishmania infantum infection status has significant impact on leishmaniasis in offspring. PLoS Negl Trop Dis. 2019;13:
e0007058 . DOIPubMedGoogle Scholar - Silva FL, Oliveira RG, Silva TM, Xavier MN, Nascimento EF, Santos RL. Venereal transmission of canine visceral leishmaniasis. Vet Parasitol. 2009;160:55–9. DOIPubMedGoogle Scholar
- Schantz PM, Steurer FJ, Duprey ZH, Kurpel KP, Barr SC, Jackson JE, et al. Autochthonous visceral leishmaniasis in dogs in North America. J Am Vet Med Assoc. 2005;226:1316–22. DOIPubMedGoogle Scholar
- Naucke TJ, Amelung S, Lorentz S. First report of transmission of canine leishmaniosis through bite wounds from a naturally infected dog in Germany. Parasit Vectors. 2016;9:256. DOIPubMedGoogle Scholar
- McGrotty Y, Kilpatrick S, Magowan D, Colville R. Canine leishmaniosis in a non-travelled dog. Vet Rec. 2023;192:174–6. DOIPubMedGoogle Scholar
- Morales-Yuste M, Martín-Sánchez J, Corpas-Lopez V. Canine leishmaniasis: update on epidemiology, diagnosis, treatment, and prevention. Vet Sci. 2022;9:387. DOIPubMedGoogle Scholar
- Esch KJ, Petersen CA. Transmission and epidemiology of zoonotic protozoal diseases of companion animals. Clin Microbiol Rev. 2013;26:58–85. DOIPubMedGoogle Scholar
- Pereira MA, Santos R, Oliveira R, Costa L, Prata A, Gonçalves V, et al. Prognostic factors and life expectancy in canine leishmaniosis. Vet Sci. 2020;7:128. DOIPubMedGoogle Scholar
- Berger BA, Bartlett AH, Saravia NG, Galindo Sevilla N. Pathophysiology of leishmania infection during pregnancy. Trends Parasitol. 2017;33:935–46. DOIPubMedGoogle Scholar
- Pineda JA, Martín-Sánchez J, Macías J, Morillas F. Leishmania spp infection in injecting drug users. Lancet. 2002;360:950–1. DOIPubMedGoogle Scholar
- Miró G, López-Vélez R. Clinical management of canine leishmaniosis versus human leishmaniasis due to Leishmania infantum: Putting “One Health” principles into practice. Vet Parasitol. 2018;254:151–9. DOIPubMedGoogle Scholar
- Franssen SU, Sanders MJ, Berriman M, Petersen CA, Cotton JA. Geographic origin and vertical transmission of Leishmania infantum parasites in hunting hounds, United States. Emerg Infect Dis. 2022;28:1211–23. DOIPubMedGoogle Scholar
- Schaut RG, Robles-Murguia M, Juelsgaard R, Esch KJ, Bartholomay LC, Ramalho-Ortigao M, et al. Vectorborne transmission of Leishmania infantum from hounds, United States. Emerg Infect Dis. 2015;21:2209–12. DOIPubMedGoogle Scholar
- Young DG. Phlebotomine sand flies of North America (Diptera: Psychodidae). Mosq News. 1984;44:2.
- McHugh CP, Grogl M, Kreutzer RD. Isolation of Leishmania mexicana (Kinetoplastida: Trypanosomatidae) from Lutzomyia anthophora (Diptera: Psychodidae) collected in Texas. J Med Entomol. 1993;30:631–3. DOIPubMedGoogle Scholar
- Beasley EA, Mahachi KG, Petersen CA. Possibility of Leishmania transmission via Lutzomyia spp. sand flies within the USA and implications for human and canine autochthonous infection. Curr Trop Med Rep. 2022;9:160–8. DOIPubMedGoogle Scholar
- Lawyer PG, Young DG. Experimental transmission of Leishmania mexicana to hamsters by bites of phlebotomine sand flies (Diptera: Psychodidae) from the United States. J Med Entomol. 1987;24:458–62. DOIPubMedGoogle Scholar
- Endris RG, Young DG, Perkins PV. Experimental transmission of Leishmania mexicana by a North American sand fly, Lutzomyia anthophora (Diptera: Psychodidae). J Med Entomol. 1987;24:243–7. DOIPubMedGoogle Scholar
- Lawyer PG, Young DG, Butler JF, Akin DE. Development of Leishmania mexicana in Lutzomyia diabolica and Lutzomyia shannoni (Diptera: Psychodidae). J Med Entomol. 1987;24:347–55. DOIPubMedGoogle Scholar
- Travi BL, Ferro C, Cadena H, Montoya-Lerma J, Adler GH. Canine visceral leishmaniasis: dog infectivity to sand flies from non-endemic areas. Res Vet Sci. 2002;72:83–6. DOIPubMedGoogle Scholar
- Courtenay O, Peters NC, Rogers ME, Bern C. Combining epidemiology with basic biology of sand flies, parasites, and hosts to inform leishmaniasis transmission dynamics and control. PLoS Pathog. 2017;13:
e1006571 . DOIPubMedGoogle Scholar - Scorza BM, Mahachi KG, Cox AC, Toepp AJ, Leal-Lima A, Kumar Kushwaha A, et al. Leishmania infantum xenodiagnosis from vertically infected dogs reveals significant skin tropism. PLoS Negl Trop Dis. 2021;15:
e0009366 . DOIPubMedGoogle Scholar - Paltrinieri S, Solano-Gallego L, Fondati A, Lubas G, Gradoni L, Castagnaro M, et al.; Canine Leishmaniasis Working Group, Italian Society of Veterinarians of Companion Animals. Guidelines for diagnosis and clinical classification of leishmaniasis in dogs. J Am Vet Med Assoc. 2010;236:1184–91. DOIPubMedGoogle Scholar
- Miró G, Wright I, Michael H, Burton W, Hegarty E, Rodón J, et al. Seropositivity of main vector-borne pathogens in dogs across Europe. Parasit Vectors. 2022;15:189. DOIPubMedGoogle Scholar
- Martín-Sánchez J, Rodríguez-Granger J, Morillas-Márquez F, Merino-Espinosa G, Sampedro A, Aliaga L, et al. Leishmaniasis due to Leishmania infantum: Integration of human, animal and environmental data through a One Health approach. Transbound Emerg Dis. 2020;67:2423–34. DOIPubMedGoogle Scholar
- Estevam LGTM, Veloso LB, Silva GG, Mori CC, Franco PF, Lima ACVMR, et al. Leishmania infantum infection rate in dogs housed in open-admission shelters is higher than of domiciled dogs in an endemic area of canine visceral leishmaniasis. Epidemiological implications. Acta Trop. 2022;232:
106492 . DOIPubMedGoogle Scholar - Hamel D, Silaghi C, Pfister K. Arthropod-borne infections in travelled dogs in Europe. Parasite. 2013;20:9. DOIPubMedGoogle Scholar
- Teske E, van Knapen F, Beijer EG, Slappendel RJ. Risk of infection with Leishmania spp. in the canine population in the Netherlands. Acta Vet Scand. 2002;43:195–201. DOIPubMedGoogle Scholar
Figures
Cite This ArticleOriginal Publication Date: November 20, 2024
1Preliminary results from this study were presented at the American Society for Tropical Medicine and Hygiene Annual Meeting; October 18–22, 2023; Chicago, Illinois, USA.
2These first authors contributed equally to this article.
3These senior authors contributed equally to this article.
Table of Contents – Volume 30, Number 12—December 2024
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
David R. Marquez, US Army Veterinary Services, 8252 Blackhawk Rd, Aberdeen Proving Ground, MD 21010, USA
Top