Volume 31, Number 7—July 2025
CME ACTIVITY - Research
Multicenter Case–Control Study of Behavioral, Environmental, and Geographic Risk Factors for Talaromycosis, Vietnam
Figure
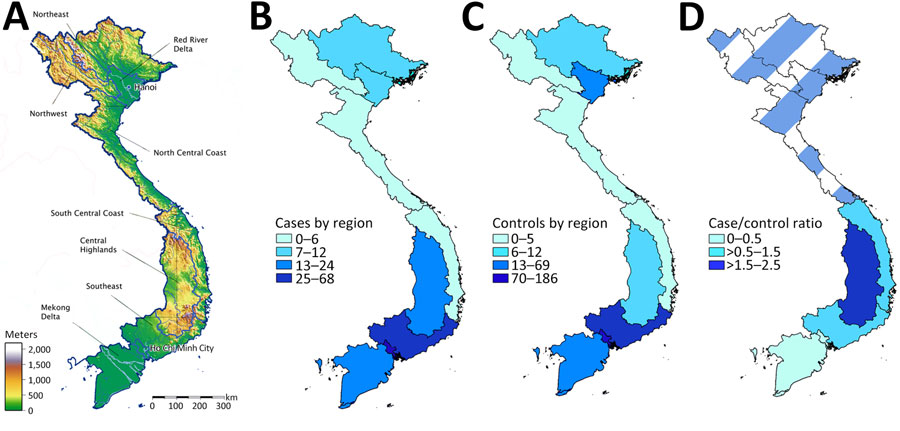
Figure. Geographic distribution of recruited cases and controls in multicenter study of behavioral, environmental, and geographic risk factors for talaromycosis, Vietnam. A) Municipal regions of Vietnam, showing topography and locations of recruitment centers in Hanoi and Ho Chi Minh City; B) number of cases by region; C) number of controls by region; D) ratio of cases to controls by region. Darker color represents a higher number of cases relative to controls for that region. A case-to-control ratio of 0.5 is expected because 2 controls were recruited for every case. A ratio <0.5 indicates a lower-than-expected number of cases relative to controls. A ratio >0.5 indicates a greater-than-expected number of cases relative to controls. Data for northern regions of Vietnam are excluded from panel D because study enrollment from these regions was insufficient to draw meaningful conclusions from the analysis. Both cases and controls are concentrated in Southern Vietnam, where most participants were recruited. The ratios of cases to controls are higher in the Central Highlands and the adjacent Southeast and South-Central Coast regions than in Ho Chi Minh City and the Mekong Delta; the highest ratio was seen in the Central Highlands region.
1These authors contributed equally to this article.