Volume 32, Number 7—July 2026
Research Letter
Ophthalmomyiasis Outbreak Caused by Oestrus ovis Infection, Algeria, 2025
Cite This Article
Citation for Media
Abstract
Ophthalmomyiasis is a rare eye infestation caused by fly larvae and more often seen in rural areas. We report an outbreak of 17 patients in Algeria with ophthalmomyiasis after sheep exposure. All patients fully recovered after removal of ocular Oestrus ovis larvae and topical therapy, highlighting the effectiveness of early detection and treatment.
Ophthalmomyiasis is a rare ocular infestation in modern clinical settings. Oestrus ovis, the sheep nasal bot fly, is the most common cause of human cases (1). Because O. ovis larvae primarily infect sheep and goats, human infection occurs predominantly in rural settings, although urban cases have been reported (2–4). Ophthalmomyiasis is classified as external, internal, or orbital, on the basis of infestation site. External ophthalmomyiasis is limited to the ocular surface, involving the conjunctiva and cornea (5). Internal ophthalmomyiasis affects intraocular structures including the anterior chamber, choroid, and vitreous (6). Last, orbital ophthalmomyiasis involves the orbital cavity and adjacent tissues. Larval migration and intraocular involvement can cause structural damage and vision loss (7).
We report a case series of 17 patients with acute external ophthalmomyiasis caused by O. ovis infection after sheep exposure during ritual sacrifice for Eid al-Adha in Algeria during June 6–8, 2025. Patients were 26–45 years of age; 10 were men and 7 were women. Sixteen patients reported exposure during Eid al-Adha, whereas 1 patient denied direct or indirect sheep exposure but suspected a foreign body in the eye. The time from exposure to hospital visit ranged from 5 to 32 hours, and symptom onset occurred 1–10 hours after exposure (Appendix Table, https://wwwnc.cdc.gov/EID/article/32/7/26-0552-App1.pdf).
Figure 1

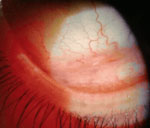
Figure 1. Clinical ocular findings in patients with acute external ophthalmomyiasis caused by Oestrus ovisinfection after sheep exposure during Eid al-Adha, Algeria, 2025. A–C) Representative external ocular photographs show acute...
Video
Video. Representative video showing Oestrus ovis larvae in patient with acute external ophthalmomyiasis caused by Oestrus ovisinfection after sheep exposure during Eid al-Adha, Algeria, 2025. Larvae exhibit...
Figure 2

Figure 2. Morphologic identification of Oestrus ovislarvae extracted from patients with acute external ophthalmomyiasis after sheep exposure during Eid al-Adha, Algeria, 2025. A, B) Extracted first-instar larva from the ocular...
Clinical manifestations included palpebral edema, conjunctival hyperemia, pruritus, foreign body sensation, epiphora, chemosis, photophobia, and pricking pain (Figure 1, panels A–C). All cases were unilateral. Slit-lamp examination revealed numerous and motile larvae on the cornea, bulbar conjunctiva, and upper and lower conjunctival fornices with active movement (Figure 1, panels D and E; Video). Conjunctivitis-like signs included conjunctival congestion or edema, mucous discharge, and punctate keratitis (Figure 1, panels F–I). Corneal impairment was observed in 10 of 17 cases, including punctate keratitis in most and epithelial defects in 3 severe cases. Larvae measured ≈1–2 mm (Figure 2, panels A, B), and 4–22 larvae were identified per affected eye. Intraocular pressure was normal in all patients. Funduscopic examination and optical coherence tomography did not reveal posterior segment abnormalities (Appendix Figure).
We rinsed and immersed extracted specimens in phosphate-buffered saline before submission for parasitologic analysis at the Parasitology Laboratory, Tongji Medical College, Huazhong University of Science and Technology (Wuhan, China). We treated the specimens with lactic acid–phenol, and microscopic examination revealed internal larval structures that included body segments, spines, spicules, cephalic oral hooks, valves (shape and number of stomata), and the cephalopharyngeal skeleton, consistent with O. ovis larvae (Figure 2, panels C–E).
We removed all visible larvae from infected patients and subsequently treated the patients with topical antimicrobial drug eye drops (4×/d for 1 wk) and neomycin/polymyxin B/dexamethasone ophthalmic ointment (1×/d for 1 wk), except in patients with corneal lesions. All patients achieved complete clinical resolution within 1–2 weeks without complications.
From our investigation, we believe that O. ovis larvae entered the patients’ eyes when adult flies deposited first-stage larvae. The substantial larval burden contributed to conjunctival inflammation and superficial corneal abrasions through cephalic oral hooks and body spicules.
O. ovis ophthalmomyiasis is traditionally associated with sheep- and goat-rearing areas in warm, dry Mediterranean climates (8). However, recent European reports (2–4) suggest broader geographic distribution; cases have been described in temperate or urban areas (9) and sometimes without clear livestock exposure. External ophthalmomyiasis might be overlooked because it closely mimics acute viral or bacterial conjunctivitis or nonspecific inflammatory ocular irritation (1,10). Thorough ocular examination and detailed livestock exposure history are therefore essential for timely diagnosis. Prompt mechanical removal of all larvae is critical to prevent intraocular involvement. This large cluster of 17 patients with ophthalmomyiasis underscores the potential for zoonotic ocular infestation from unprotected sheep contact during seasonal religious rituals. Public education, eye protection, and hygiene practices during ritual slaughter might help reduce similar outbreaks in endemic regions.
Dr. Zeng is a clinician-scientist in the Department of Ophthalmology at Stanford University School of Medicine and an ophthalmologist with residency training in ophthalmology. Her research focuses on translational studies of a broad range of eye diseases, including glaucoma, therapeutic strategies to protect retinal ganglion cells and preserve vision, retinal neurodegeneration, and ocular infectious diseases.
Acknowledgments
We thank the administration and clinical staff of El Moudjahid Madjen Benmira Hospital for their support in enabling this study. We also acknowledge the patients who participated and contributed to this research.
This work was supported by the Open Research Fund of Hubei Key Laboratory (award no. 2021KFY057 to Y.Z.).
References
- Martinez-Rojano H, Huerta H, Sámano R, Chico-Barba G, Mier-Cabrera J, Plascencia-Nieto ES. Ophthalmomyiasis externa and importance of risk factors, clinical manifestations, and diagnosis: review of the medical literature. Diseases. 2023;11:180. DOIPubMedGoogle Scholar
- Tamponi C, Pasini C, Ahmed F, Dessì G, Contu E, Porcu F, et al. External ophthalmomyiasis by Oestrus ovis in tourists visiting Italy. Report of three cases and a literature review. Travel Med Infect Dis. 2022;46:
102279 . DOIPubMedGoogle Scholar - Vedpathak M, Chatterjee N, Baradkar V, Shastri J. Ophthalmomyiasis externa: a case report. Trop Parasitol. 2020;10:147–9. DOIPubMedGoogle Scholar
- Rosenberg R, Halimi E, Benayoun Y, Khadimallah Y, Robert PY. External ophthalmomyiasis (botfly larval infestation) in urban France [In French]. J Fr Ophtalmol. 2013;36:466–7.PubMedGoogle Scholar
- Abihaidar N, Garcin T. External ophthalmomyiasis due to Oestrus ovis. N Engl J Med. 2022;386:
e35 . DOIPubMedGoogle Scholar - Rodger DC, Kim EL, Rao NA. Ophthalmomyiasis interna. Ophthalmology. 2016;123:247.PubMedGoogle Scholar
- Singh P, Tripathy K. Ophthalmomyiasis. StatPearls. 2023 [cited 2025 Aug 25]. https://www.ncbi.nlm.nih.gov/books/NBK576408
- Dunbar J, Cooper B, Hodgetts T, Yskandar H, van Thiel P, Whelan S, et al. An outbreak of human external ophthalmomyiasis due to Oestrus ovis in southern Afghanistan. Clin Infect Dis. 2008;46:e124–6.PubMedGoogle Scholar
- D’Assumpcao C, Bugas A, Heidari A, Sofinski S, McPheeters RA. A case and review of ophthalmomyiasis caused by Oestrus ovis in the central valley of California, United States. J Investig Med High Impact Case Rep. 2019;7:
2324709619835852 .PubMedGoogle Scholar - Balamurugan R, Gupta PC, Dhingra D, Ram J. External ophthalmomyiasis by Oestrus ovis larvae. QJM. 2020;113:751.PubMedGoogle Scholar
Figures
Cite This ArticleOriginal Publication Date: June 24, 2026
1These first authors contributed equally to this article.
Table of Contents – Volume 32, Number 7—July 2026
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Yunyun Zhou, Renmin Hospital of Wuhan University, 238 Jiefang Rd, Wuchang District, Wuhan, Hubei 430060, China
Top