Volume 32, Number 7—July 2026
Synopsis
Neurosurgical Biopsy and Resection for Diagnosis and Treatment of Balamuthia mandrillaris Amebic Encephalitis, United States
Figure 1
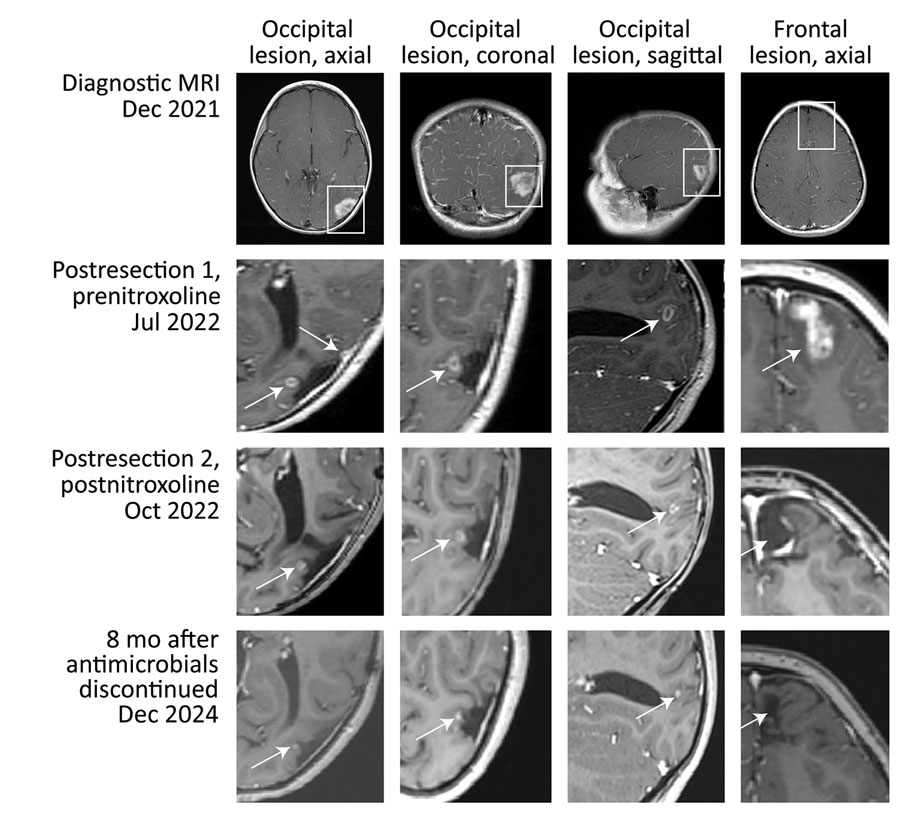
Figure 1. Axial, coronal, and sagittal postcontrast T1-weighted MRI images from study of neurosurgical biopsy and resection for diagnosis and treatment of Balamuthia mandrillaris amebic encephalitis, United States. Top row images show patient’s primary occipital and frontal lesions (boxes). Three weeks after resection of the first occipital lesion (second row), recurrent nodules (arrows) developed around the resection cavity. Before nitroxoline initiation, those nodules were enlarging. MRI in July 2022 (second row) showed a new, 7-mm diameter, indistinct, fluid attenuated inversion recovery–hyperintense, enhancing focus in the anterior aspect of the left superior frontal gyrus. After nitroxoline (third row), the occipital lesions retracted (arrows) and were no longer ring-enhancing. No recurrent lesions were noted at the resection site of the frontal lesion, which was resected while the patient was on multidrug therapy and 4 weeks before starting nitroxoline. Follow-up imaging 8 months after antimicrobial treatment was discontinued (fourth row), a stable, residual nodule (arrows) in the medial resection cavity remained, thought to represent gliosis. MRI, magnetic resonance imaging.
1These authors contributed equally to this article.