Volume 32, Number 7—July 2026
Synopsis
Neurosurgical Biopsy and Resection for Diagnosis and Treatment of Balamuthia mandrillaris Amebic Encephalitis, United States
Figure 2
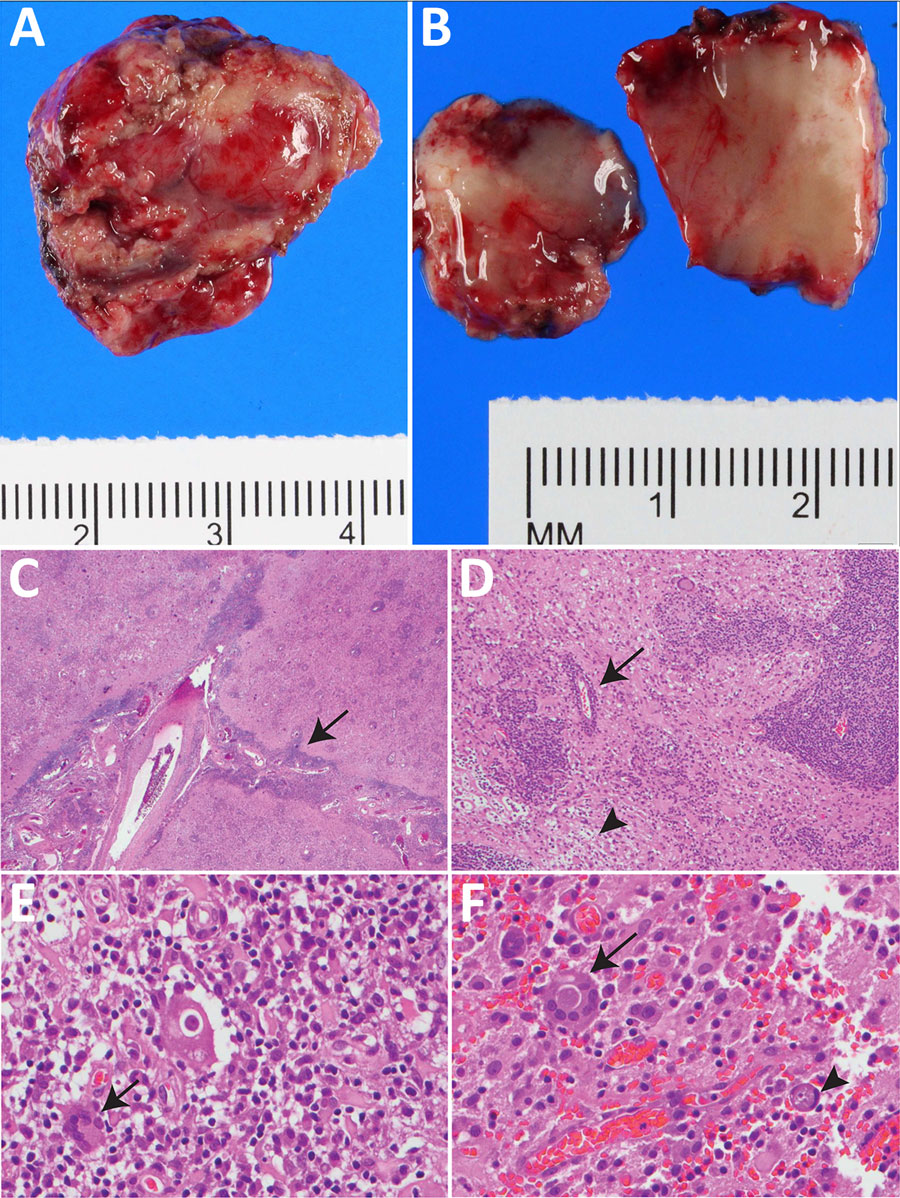
Figure 2. Resected occipital lesion gross and histopathology from patient in study of neurosurgical biopsy and resection for diagnosis and treatment of Balamuthia mandrillaris amebic encephalitis, United States. A) Gross pathology revealed pink-tan, firm tissue fragments. B) Cut sections reveal a heterogenous, tan-pink, and soft surface with effacement of the white and gray matter demarcation. C, D) Hematoxylin and eosin stained sections of the brain show leptomeningeal thickening with striking perivascular lymphocytic infiltrate (C, arrow) extending into the cortical parenchyma with foci of lymphocytic infiltration into the vessel wall, consistent with vasculitis (D, arrow). The architecture of the cortical gray matter is obliterated by neuronal loss, reactive gemistocytic astrocytes and infiltration by macrophages, multinucleated giant cells, and lymphocytes. This involves the adjacent white matter with areas of parenchymal loss/liquefactive necrosis (D, arrowhead). Original magnification ×2 for panel C, ×10 for panel D. E, F) Many of the multinucleated giant cells (E, arrow) contain large round thick-walled parasites (F, arrow) containing granular material and an occasional inconspicuous, dot like nucleus (F, arrowhead). Original magnification ×40 for panels E and F. Occasional structures resembling engulfed organisms are seen in the parenchyma (D–F).
1These authors contributed equally to this article.