Volume 32, Number 7—July 2026
Synopsis
Neurosurgical Biopsy and Resection for Diagnosis and Treatment of Balamuthia mandrillaris Amebic Encephalitis, United States
Figure 3
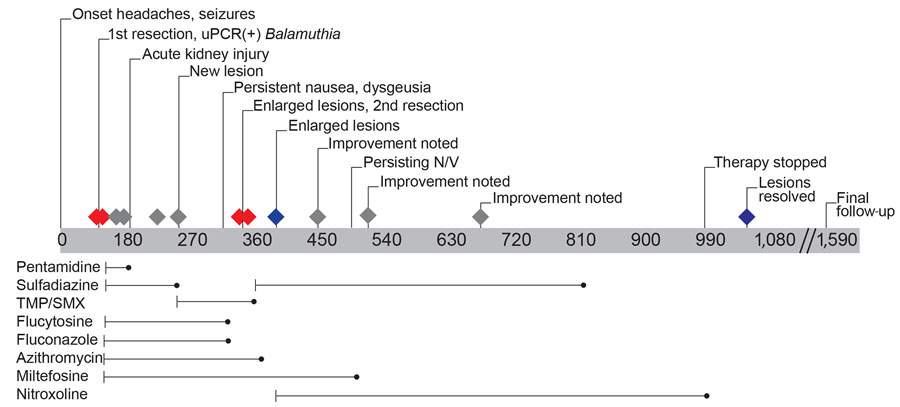
Figure 3. Timeline of events and medications for patient in study of neurosurgical biopsy and resection for diagnosis and treatment of Balamuthia mandrillaris amebic encephalitis, United States. Gray bar shows days since initial evaluation; red diamonds indicate magnetic resonance imaging (MRI) obtained before and after surgical dates; gray diamonds indicate interval MRI; blue diamonds indicate MRI before and after end date of nitroxoline. Nitroxoline dosing was titrated over 1 week to a total of 30 mg/kg/day 3 times/day; other medication dosing was pentamidine, 4 mg/kg (80 mg) every 24 hours; sulfadiazine, 50 mg/kg (1,000 mg) every 6 hours; azithromycin, 20 mg/kg (400 mg) every 24 hours; fluconazole, 12 mg/kg (240 mg) every 24 hours; flucytosine, 37.5 mg/kg (750 mg) every 6 hours; and miltefosine, 2.5 mg/kg (50 mg) every 24 hours. Pentamidine was discontinued after 8 weeks because of concern for renal toxicity. Sulfadiazine was briefly switched to trimethoprim/sulfamethoxazole because of manufacturer supply shortage and ultimately discontinued because of cost and administration concerns. Because of persistent nausea, vomiting, dysgeusia, and anorexia, flucytosine, fluconazole, azithromycin, and miltefosine were each discontinued, and the patient remained on nitroxoline for a total of 19 months. N/V, nausea and vomiting; TMP/SMX, trimethoprim/sulfamethoxazole; uPCR, universal broad-range PCR amplicon sequencing.
1These authors contributed equally to this article.