Volume 32, Number 7—July 2026
Synopsis
Neurosurgical Biopsy and Resection for Diagnosis and Treatment of Balamuthia mandrillaris Amebic Encephalitis, United States
Cite This Article
Citation for Media
Abstract
We report a systematic case review of antemortem neurosurgical resections and biopsies and outcomes including new lesions after procedure and survival in Balamuthia mandrillaris granulomatous amebic encephalitis. The investigation was prompted by a 5-year-old patient in the southwestern United States who was treated with nitroxoline, the 2021 Centers for Disease Control and Prevention regimen, and underwent 2 resections; initial resection site recurrence and a new lesion after resection prompted the question whether complete resection versus biopsy is associated with better outcomes. We conducted a literature review and found no substantial difference between neurosurgical resection versus biopsy-only groups. Limitations include case review, number of cases, and incomplete data available. Additional analyses comparing neurosurgical outcomes with outcomes of those diagnosed via blood or cerebrospinal fluid and metagenomic next-generation sequencing might provide more definitive answers. This case and systematic review provide evidence that treatment with nitroxoline and neurosurgical resection could contribute to survival in Balamuthia encephalitis case-patients.
Free-living amebae (FLA) are soil- and water-dwelling unicellular organisms found throughout the world that cause rare but often fatal infections (1,2). Acanthamoeba and Balamuthia are 2 genera of FLA that cause granulomatous amebic encephalitis (GAE), a subacute disease characterized by focal neurologic deficits, altered mental status, and >1 parenchymal brain lesions on imaging. The true incidence is unclear because of diagnostic and reporting limitations, but in the United States, <20 cases are reported annually; however, >90% of infected patients who have central nervous system (CNS) involvement die (1,2).
Acanthamoeba spp. FLA primarily affect immunocompromised hosts, whereas Balamuthia mandrillaris amebae also infect immunocompetent hosts. Balamuthia spp. amebae exist as environmentally stable cysts and infectious trophozoites, entering the body through the respiratory tract or open skin wounds and spreading hematogenously to the organs, most notably the brain (2–9). Balamuthia was first identified in a pregnant mandrill (Papio sphinx) in 1990, but as a result, posthumous human diagnoses were made dating back to 1974 (10). Since then, B. mandrillaris GAE cases have been diagnosed worldwide, many among children, and often with fatal outcomes. A review of 109 US cases during 1974–2016 revealed a 90% mortality rate (2). Even when infections are diagnosed antemortem and patients receive antiamebic medications, the fatality rate exceeds 75% (11).
The Centers for Disease Control and Prevention (CDC) recommends a regimen for B. mandrillaris GAE including pentamidine, sulfadiazine, azithromycin or clarithromycin, a triazole, flucytosine, and miltefosine (12). In 2025, CDC added nitroxoline to the recommended regimen (12). A study published in 2018 screened 2,177 clinically approved compounds (including the CDC-recommended regimen) for in vitro activity against B. mandrillaris amebae (13). A quinoline antibiotic, nitroxoline, was found to be the most potent and selective of all agents tested (including the drugs in the recommended regimen) against both cystic and trophozoite forms and at pharmacologically relevant concentrations (13). Nitroxoline has been used with a favorable side effect profile for human urinary tract infection treatment since the 1970s, including in pediatric patients (14). In 2021, an adult patient treated with nitroxoline for Balamuthia GAE survived (15). Herein, we describe a pediatric patient successfully treated with a combination of nitroxoline, the 2021 CDC recommended regimen, and 2 neurosurgical resections. We also conducted a literature review of previously published cases to determine any difference between neurosurgical resection versus biopsy-only groups.
Figure 1

Figure 1. Axial, coronal, and sagittal postcontrast T1-weighted MRI images from study of neurosurgical biopsy and resection for diagnosis and treatment of Balamuthia mandrillarisamebic encephalitis, United States. Top row images...
In autumn 2021, a previously healthy 5-year-old was brought to care with new-onset seizures and headaches. Persisting symptoms prompted brain magnetic resonance imaging (MRI), revealing a heterogeneously enhancing cortical mass at the junction between the left temporal and occipital lobes with a large region of surrounding T2 fluid attenuated inversion recovery (FLAIR) hyperintensity (Figure 1).
Figure 2
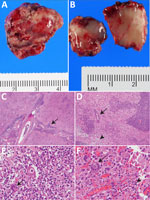
Figure 2. Resected occipital lesion gross and histopathology from patient in study of neurosurgical biopsy and resection for diagnosis and treatment of Balamuthia mandrillarisamebic encephalitis, United States. A) Gross pathology...
With malignant tumor on the differential diagnosis, the patient underwent left occipital craniotomy and the specimen was removed en bloc and sent to pathology. The neurosurgeon chose resection margins on the basis of intraoperative frameless stereotactic navigation and the appearance and feel of normal-appearing, soft, edematous brain. Postoperative MRI confirmed an enhancing mass with no change in the surrounding edema. The neurosurgery team consulted the pediatric infectious diseases service because the preliminary pathology report was concerning for infection rather than tumor. We suspected Balamuthia GAE because of course chronicity, immunocompetent host, and extensive soil exposures, including making mudpies. However, we also considered in the initial consultation Acanthamoeba (considered less likely because the patient was immunocompetent), Naegleria (considered less likely because the patient had no typical acute manifestations), mycobacterial diseases including nontuberculous (NTM) and tuberculosis (TB) (considered less likely because the patient was immunocompetent [NTM] and had no specific exposure [TB]), and endemic fungal infections with spread to the CNS (again considered less likely because the patient was immunocompetent). Histopathology revealed leptomeningeal lymphocytic infiltrate extending into the cortical parenchyma with focal vasculitis, along with lymphocytes and multinucleated giant cells containing large, round, thick-walled parasites, consistent with GAE (Figure 2). Special tissue stains were negative for acid-fast bacillus and fungal elements, but a sample of brain tissue sent to CDC’s Free-living and Intestinal Amebas laboratory (National Center for Emerging and Zoonotic Infectious Diseases, Division of Foodborne, Waterborne, and Environmental Diseases) was positive for B. mandrillaris amebae by PCR (24).
Figure 3

Figure 3. Timeline of events and medications for patient in study of neurosurgical biopsy and resection for diagnosis and treatment of Balamuthia mandrillarisamebic encephalitis, United States. Gray bar shows days...
On the basis of CDC recommendations at diagnosis, the patient was started on pentamidine (4 mg/kg [80 mg] every 24 h), sulfadiazine (50 mg/kg [1,000 mg] every 6 h), azithromycin (20 mg/kg [400 mg] every 24 h), fluconazole (12 mg/kg [240 mg] every 24 h), flucytosine (37.5 mg/kg [750 mg] every 6 h), and miltefosine (2.5 mg/kg [50 mg] every 24 h) (Figure 3). On this regimen, 5 months later, new frontal headaches developed. Repeat MRI at that time showed a new, 7-mm diameter, enhancing focus in left superior frontal gyrus and 3 enhancing nodules at the peripheral resection margins of the primary left occipital site. The multidrug regimen was continued, and repeat MRI 2 months later showed interval increase in the size of the left frontal lesion and surrounding T2/FLAIR hyperintensity (Figure 1). The patient subsequently underwent a left frontal craniotomy for en bloc resection using intraoperative frameless stereotactic navigation. Intraoperative ultrasound revealed no residual hyperechoic tissue. Pathology resembled first resection, and the tissue was again positive for B. mandrillaris amebae by PCR testing at CDC.
Given concern for progressive disease on existing therapy, along with promising in vitro data and a published successful case report (13,15), we decided to add nitroxoline to the regimen. We obtained Institutional review board approval, Food and Drug Administration emergency investigational drug designation, and parental consent. After emergency designation, we identified a foreign nitroxoline manufacturer. However, because the patient’s imaging and clinical status were worsening and obtaining the drug directly from the manufacturer would have meant a delay of several weeks, to ensure timely administration, we procured a small supply from the same manufacturer via University of California San Francisco Investigational Drug Services. The patient received the first dose of nitroxoline 1 month after second resection. We sourced subsequent treatment directlyfrom the manufacturer and established a formal contractual agreement to secure ongoing access to the investigational agent.
While monitoring the patient in the hospital for both medication side effects and worsening symptoms, we titrated the nitroxoline dose over 1 week to a total of 30 mg/kg/day (3×/d). We chose that dose because it is the maximum pediatric dose described in published nitroxoline reviews and was comparable to dosing used for an adult B. mandrillaris patient treated with nitroxoline (14,15). Clinical, laboratory, electrocardiogram, and dental monitoring showed that the patient tolerated nitroxoline without substantial side effects.
MRI at 6 weeks after nitroxoline initiation showed considerable improvement in the ring-enhancing lesions at the margin of the left occipital surgical cavity, no recurrence of left frontal lesion, and no new lesions. Her next MRI scans, at 3 and 9 months after nitroxoline initiation, showed continued improvement in the ring-enhancing lesions of the occipital region and no new lesions. MRI 1 year after nitroxoline initiation showed expected encephalomalacia and gliosis at previous resection cavities, resolution of ring-enhancing occipital lesions, and no new lesions. In total, the patient was treated for 2 years and 4 months with antiamebic therapy, including nitroxoline for the final 19 months of therapy. At 8 months after therapy ended, a tiny residual nodule in the medial resection cavity was stable and thought to represent gliosis (Figure 1). Clinical follow-up 4 years after diagnosis revealed a healthy, active child without focal neurologic findings but with mild neurocognitive and learning delays on neuropsychiatric testing.
The progression of disease and need for a second resection in this case raised the question whether complete resection, versus biopsy only, might be beneficial to outcomes of B. mandrillaris GAE. We hypothesized that because of the prevalence of vasculitis in and proposed hematogenous spread of Balamuthia disease, biopsy might promote spread by disruption of the blood–brain barrier and transection of affected vessels, whereas complete resection, aided by reducing the burden of organisms, could be associated with better outcomes. To evaluate that possibility, we performed a systematic review of the literature according to the guidelines for Preferred Reporting Items for Systematic Reviews and Meta-Analyses (16,17). We searched for published articles via PubMed (last reverified 2026 Jun 4) to identify cases in which B. mandrillaris GAE was diagnosed using specimens obtained antemortem via neurosurgical procedures, including complete resection (group 1) or subtotal resection or biopsy (group 2). We used the following search terms: Balamuthia AND (biopsy OR neurosurgery OR neurosurgical OR excision OR resection OR brain mass OR tumor). That initial search returned 231 articles (Appendix 1 Table 1). We then filtered the list by English language to 223 articles and then further filtered for human cases, bringing the number of articles to 161. We also found 6 published articles not captured in the PubMed search (15,18–23); all were noted in the course of reviewing other articles and considered pertinent to this topic. However, noting the absence of those articles in the PubMed search, to avoid omission of articles or bias, we reviewed the nonhuman filtered cases to identify erroneously omitted cases and conducted another search using terms “Balamuthia AND case report.” Those searches identified no additional articles that did not meet exclusion criteria. In total, we reviewed 168 articles (Appendix 1 Table 2).
This study was confined to antemortem neurosurgical procedures only because of the hypothesis that cutting into diseased tissue without (presumptively) substantially diminishing the burden of ameba might worsen disease outcomes in Balamuthia GAE. Therefore, we excluded the following types of cases: no neurosurgical specimen obtained antemortem (n = 36), only cutaneous disease (n = 3), infection not verified by the definitions we devised or cases of other FLA (n = 3), and co-infections (which might alter the pathogenesis) (n = 2). We also excluded the following types of studies: primary purpose of subject review (n = 30), in vitro studies (n = 22), primary purpose to report specimen data or imaging findings without substantial clinical descriptions (n = 7), environmental specimens (n = 5), duplicated cases (n = 4), editorials (n = 2), mouse studies (n = 1), nonhuman cases (n = 1), retracted articles (n = 1), articles for which we could not obtain the full text (n = 1), or case reports that did not include the targeted data (n = 1) (Appendix 1 Table 3).
We defined a confirmed case of B. mandrillaris GAE as a patient with clinical encephalitis with imaging findings supportive of diagnosis and either molecular diagnostics (PCR or metagenomic next-generation sequencing; Karius, https://kariusdx.com) or immunofluorescence or immunohistochemistry staining positive on pathologic specimens for B. mandrillaris. Cases that had only positive serologic results or morphologic evidence of ameba were not considered diagnostic for B. mandrillaris GAE.
We defined resection cases as cases in which the article defined the procedure as resection or complete excision or en bloc in an antemortem neurosurgical procedure. We defined biopsy cases as cases in which the article reported biopsy, excisional biopsy, or subtotal resection of the lesion in an antemortem neurosurgical procedure. Cases involving only blood, cerebrospinal fluid (CSF) specimens, or skin or other organ biopsies were outside the scope of this study.
We reviewed and extracted data from the 68 articles meeting inclusion and exclusion criteria. Of those, 20 were resection cases; data collected included clinical manifestation description (country of residence, age, sex, initial symptoms, notable medical history), number and location of lesions at evaluation, site of lesion resected, antiamebic medications (if used and with details to the extent published), presence of vasculitis on biopsy, additional lesions identified after procedure, and use of steroids before Balamuthia diagnosis. The remaining 48 articles were on biopsy cases; data collected included clinical manifestation description, whether >1 lesion was present at diagnosis, whether additional lesions were identified after procedure, and whether steroids were used before Balamuthia diagnosis.
For resection and biopsy studies including resection cases, we recorded the number that had additional lesions identified on brain imaging (most advanced obtained, either computed tomography or MRI) after the antemortem neurosurgical specimen collection. We also recorded the number for whom steroids were reported to be given and the number who survived the infection. For the steroid use and survival analyses, we calculated percentages on the basis of the total number of resection cases or biopsy cases. For the lesion number analysis, the denominator was the number of cases for which information was available by imaging reports, because some patients died before follow-up imaging after the procedure could be obtained.
We used GraphPad Prism (https://www.graphpad.com) for statistical analysis. We examined for statistical differences between resection cases and biopsy cases using Fisher exact tests.
From our systematic review of the literature, plus the case we report here, we found 7 published articles describing 1 or 2 cases of B. mandrillaris intracranial lesions that were surgically resected and the patient survived (18,19,25–29). Of 13 cases in which the patient subsequently died, each was associated with >1 of the following: multiple CNS lesions at initial evaluation (n = 5) (Appendix 2 Table 1 references 5,17–19), advanced neurologic symptoms (i.e., hemiparesis, seizures, signs of increased intracranial pressure or herniation, loss of consciousness) (n = 9) (Appendix 2 Table 1 references 5,6,10,13,17–19), vasculitis on imaging or pathology (n = 5) (Appendix 2 Table 1 references 5–7,10,17), a regimen distinct from the 2021 CDC medication regimen (<4 agents used) (n = 11) (Appendix 2 Table 1, references 5–7,12,13,16–19), or steroid use preceding diagnosis and antiamebic treatment (n = 6) (Appendix 2 Table 1 references 5,10,12,17-19).
We questioned whether resection, either subtotal or biopsy or complete resection, increased likelihood of patient death or additional lesions arising after the neurosurgical procedure. Vasculitis is a prominent feature of B. mandrillaris GAE (30). We hypothesized that incision into infected tissue might promote spread of ameba if total resection is not achieved. Therefore, we conducted an additional review of the cases that had biopsy or subtotal resections for outcomes of survival or death and whether additional lesions were discovered on follow-up imaging after the procedure. We found no statistical difference between the groups, however (Table; Appendix 2 Table 2), and similar rates of steroid use before B. mandrillaris GAE diagnosis.
We report the excellent outcome for a pediatric patient with B. mandrillaris GAE treated with nitroxoline. Factors contributing to GAE survival are not clear, but we believe that nitroxoline and neurosurgical interventions were important to this patient’s survival. A multidisciplinary team, including pharmacy, psychology, and child life services, individualized the patient’s complex medication schedule, which, along with family vigilance, undoubtedly contributed to the success of this regimen. Our findings of clinical and radiographic improvement add to a growing body of literature suggesting that nitroxoline, in combination with other antiamebic drugs and surgical resection, could improve outcomes from this rare, highly fatal disease. Nitroxoline has better tolerability and in vitro efficacy against B. mandrillaris infection than other antiamebic agents (13,31). In a review of safety and efficacy of nitroxoline in UTI treatment, only 9.8% of patients reported adverse effects (primarily nausea) (13,14,31). In contrast, the standard regimen, which includes pentamidine, miltefosine, a triazole, flucytosine, azithromycin, and sulfadiazine, has substantial toxicities, often limiting use and leading to other adverse conditions. Indeed, acute kidney injury and hypertension occurred in this patient, but resolved after discontinuation of pentamidine. In addition, gastrointestinal side effects of dysgeusia, anorexia, nausea, vomiting, and diarrhea necessitated placing a gastrostomy tube for nutrition; those symptoms resolved after sequential discontinuation of miltefosine, fluconazole, flucytosine, and azithromycin and did not recur during nitroxoline monotherapy.
Nitroxoline was continued throughout the final 19 months’ duration of this patient’s antiamebic therapy, and clinical and radiographic improvement continued even during the final 6 months on nitroxoline monotherapy, suggesting that nitroxoline could be a contributor to her survival. Our review of the literature subsequent to this case identified 2 other reported uses of nitroxoline, in addition to the adult case reported in the introduction (15). Those 2 cases were pediatric as well, but neither included neurosurgical resection. In the first case, a 4-year-old had B. mandrillaris infection diagnosed by Karius testing of blood and confirmed by CSF PCR. Nitroxoline was started 1 month into diagnosis, but the patient died 1 month later (32). The other pediatric case, in a 2-year-old, was diagnosed by biopsy and was included in this systematic review; the patient survived, as reported at 1 year after manifestation (33).
We cannot definitively determine the independent contribution of nitroxoline to treatment success on the basis of the case we report or the few others that have been published. However, a lack of recurrence or progression over a period of 19 months on nitroxoline, including 6 months of nitroxoline alone, supports the possibility that nitroxoline contributed to recovery. Before nitroxoline was initiated, testing showed a new frontal lesion and progression of that lesion (Figures 1, 3), but after nitroxoline treatment began, no new progression or lesions developed, and occipital residual lesions shrank. In addition, at the resection margins of the frontal lesion addressed in the second resection, surrounding residual nodules did not develop during nitroxoline treatment, unlike after the first resection before nitroxoline treatment. Variations in the success of complete resection microscopically, brief steroid use postoperatively after first resection, and being on any antiamebic therapy at the second resection all likely contributed as well.
The role of neurosurgical intervention for Balamuthia infections remains unclear. Whereas Karius testing and metagenomic next-generation sequencing can provide new opportunities for diagnosis without neurosurgical intervention (20,32,34–42), brain biopsy can lead to definitive diagnosis and early therapy. However, few cases manifest with lesions amenable to complete resection (18,19,25–29). Lesion recurrence after this patient’s first surgery, despite using the CDC-recommended regimen, suggests that infection might have extended into normal-appearing tissue, beyond resection margins (i.e. incomplete resection); the previous CDC-recommended regimen could be insufficient to treat Balamuthia GAE; or vasculitis or resection in the setting of steroids or vasculitis without concurrent medication against Balamuthia amebae might contribute to dissemination (30). Of interest, we saw no recurrence from the patient’s second resection, but at that time, the patient had concurrent treatment with antiamebic medications, including nitroxoline shortly thereafter. Our review and analyses suggest that variations in completeness of excision might not determine the recurrence or development of new lesions because no substantial difference in new lesions after biopsy or resection were noted between the 2 groups. We did find a trend toward association of excision with survival that warrants further investigation; however, the data did not show a statistically significant survival benefit to excision.
Our study is limited by the nature of literature reviews, including incomplete information and relatively small numbers, given the rarity of the disease. For example, with respect to steroid use, some articles (3 cases of the biopsy-only group) reported that the patients were initially treated for CNS TB. Providing steroids is the standard of care for such cases, so the lack of steroids reported in many of those cases exemplifies possible missing data in the literature (43). Future studies comparing the outcomes of patients who have antemortem neurosurgical resections or biopsies with those who only have non-CNS procedures for diagnosis or therapy (i.e., skin biopsies, blood or CSF specimens only) will be further informative on the risks of neurosurgical intervention in Balamuthia GAE. In addition to that theorized risk, risks of neurosurgery must always be considered before surgical intervention, but lack of recurrent or new lesions in this patient case report after the second resection might have been the result of the multidrug regimen used before resection, and the addition of nitroxoline shortly after resection.
In this systematic review and analysis, we found no statistically significant outcomes between the group for whom biopsy was conducted for diagnosis and the group for whom complete resection for diagnosis and therapy was used. However, we did find a trend toward benefit in survival in complete resection group that warrants further study.
In conclusion, we report a systematic review of survival in B. mandrillaris GAE after antemortem neurosurgical resections and biopsies, including successful treatment of a pediatric patient in the southwestern United States. For patients with B. mandrillaris GAE, neurosurgical management, multidrug therapy, and nitroxoline treatment could improve outcomes associated with this deadly infection.
Dr. Rubbab is an assistant professor of pediatrics in the Division of Infectious Diseases at Baylor College of Medicine. Her clinical and research interests include pediatric infectious diseases, antimicrobial stewardship, infections in immunocompromised children, and improving patient safety. Dr. Adenwalla is a neurosurgery resident at UT Southwestern Medical Center. His work centers on neurosurgical outcomes and surgical innovation, with a particular interest in advancing techniques that improve patient care.
Acknowledgments
We thank the patient and the family for participating in this study. The parents gave written consent to the publication of the patient’s clinical manifestations, treatment, and follow-up as described in this manuscript. Asieris Pharmaceuticals provided nitroxoline. We appreciate the advice and guidance of Joseph L. DeRisi and the information received by direct communication from Joshua Cuoco.
This activity was reviewed by CDC and was conducted consistent with applicable federal law and CDC policy. See e.g., 45 C.F.R. part 46.102(I)(2), 21 C.F.R. part 56; 42 U.S.C. §241(d); 5 U.S.C. §552a; 44 U.S.C. §3501 et seq. The University of Texas Southwestern Medical Center Institutional Review Board reviewed and approved use of nitroxoline for this patient.
The authors acknowledge using ChatGPT in this manuscript for the sole purpose of assistance in concise wording, not in a generative capacity.
References
- Haston JC, O’Laughlin K, Matteson K, Roy S, Qvarnstrom Y, Ali IKM, et al. The epidemiology and clinical features of non-keratitis Acanthamoeba infections in the United States, 1956–2020. Open Forum Infect Dis. 2023;10:
ofac682 . DOIPubMedGoogle Scholar - Cope JR, Landa J, Nethercut H, Collier SA, Glaser C, Moser M, et al. The epidemiology and clinical features of Balamuthia mandrillaris disease in the United States, 1974–2016. Clin Infect Dis. 2019;68:1815–22. DOIPubMedGoogle Scholar
- Martinez AJ, Visvesvara GS. Free-living, amphizoic and opportunistic amebas. Brain Pathol. 1997;7:583–98. DOIPubMedGoogle Scholar
- Shehab KW, Aboul-Nasr K, Elliott SP. Balamuthia mandrillaris granulomatous amebic encephalitis with renal dissemination in a previously healthy child: case report and review of the pediatric literature. J Pediatric Infect Dis Soc. 2018;7:e163–8. DOIPubMedGoogle Scholar
- Matin A, Siddiqui R, Jayasekera S, Khan NA. Increasing importance of Balamuthia mandrillaris. Clin Microbiol Rev. 2008;21:435–48. DOIPubMedGoogle Scholar
- Siddiqui R, Matin A, Warhurst D, Stins M, Khan NA. Effect of antimicrobial compounds on Balamuthia mandrillaris encystment and human brain microvascular endothelial cell cytopathogenicity. Antimicrob Agents Chemother. 2007;51:4471–3. DOIPubMedGoogle Scholar
- Matin A, Siddiqui R, Jung SY, Kim KS, Stins M, Khan NA. Balamuthia mandrillaris interactions with human brain microvascular endothelial cells in vitro. J Med Microbiol. 2007;56:1110–5. DOIPubMedGoogle Scholar
- Matin A, Stins M, Kim KS, Khan NA. Balamuthia mandrillaris exhibits metalloprotease activities. FEMS Immunol Med Microbiol. 2006;47:83–91. DOIPubMedGoogle Scholar
- Jayasekera S, Matin A, Sissons J, Maghsood AH, Khan NA. Balamuthia mandrillaris stimulates interleukin-6 release in primary human brain microvascular endothelial cells via a phosphatidylinositol 3-kinase-dependent pathway. Microbes Infect. 2005;7:1345–51. DOIPubMedGoogle Scholar
- Visvesvara GS, Martinez AJ, Schuster FL, Leitch GJ, Wallace SV, Sawyer TK, et al. Leptomyxid ameba, a new agent of amebic meningoencephalitis in humans and animals. J Clin Microbiol. 1990;28:2750–6. DOIPubMedGoogle Scholar
- Spottiswoode N, Haston JC, Hanners NW, Gruenberg K, Kim A, DeRisi JL, et al. Challenges and advances in the medical treatment of granulomatous amebic encephalitis. Ther Adv Infect Dis. 2024;11:
20499361241228340 . DOIPubMedGoogle Scholar - Centers for Disease Control and Prevention. Clinical care of Balamuthia infection. 2025 [cited 2025 Apr 1]. https://www.cdc.gov/balamuthia/hcp/clinical-care
- Laurie MT, White CV, Retallack H, Wu W, Moser MS, Sakanari JA, et al. Functional assessment of 2,177 U.S. and international drugs identifies the quinoline nitroxoline as a potent amoebicidal agent against the pathogen Balamuthia mandrillaris. MBio. 2018;9:e02051–18. DOIPubMedGoogle Scholar
- Naber KG, Niggemann H, Stein G, Stein G. Review of the literature and individual patients’ data meta-analysis on efficacy and tolerance of nitroxoline in the treatment of uncomplicated urinary tract infections. BMC Infect Dis. 2014;14:628. DOIPubMedGoogle Scholar
- Spottiswoode N, Pet D, Kim A, Gruenberg K, Shah M, Ramachandran A, et al. Successful treatment of Balamuthia mandrillaris granulomatous amebic encephalitis with nitroxoline. Emerg Infect Dis. 2023;29:197–201. DOIPubMedGoogle Scholar
- Page MJ, Moher D, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021;372. DOIPubMedGoogle Scholar
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372. DOIPubMedGoogle Scholar
- Mei J, Sheng F, Zhang C, Chen X. Imaging monitoring of Balamuthia granulomatous amoebic encephalitis. Clin Neurol Neurosurg. 2025;254:
108917 . DOIPubMedGoogle Scholar - Lehmer LM, Ulibarri GE, Ragsdale BD, Kunkle J. Cutaneous Balamuthia mandrillaris infection as a precursor to Balamuthia amoebic encephalitis (BAE) in a healthy 84-year-old Californian. Dermatol Online J. 2017;23:13030/qt8c8720qm. DOIPubMedGoogle Scholar
- Edminster SY, Rebbe RW, Khatchadourian C, Hurth KM, Mathew AJ, Huss-Bawab J, et al. The role of plasma metagenomic sequencing in identification of Balamuthia mandrillaris encephalitis. Acta Neuropathol Commun. 2025;13:60. DOIPubMedGoogle Scholar
- Tello-Zavala MC, Bravo-Oro A, Falcón-Escobedo R. Central nervous system infection in an immunocompetent Mexican child. Pediatr Infect Dis J. 2014;33:991, 995–6.PubMedGoogle Scholar
- Li Q, Yang XH, Qian J. September 2004: a 6-year-old girl with headache and stiff neck. Brain Pathol. 2005;15:93–5. DOIPubMedGoogle Scholar
- Atay Ünal N, Kuzucu P, Bedir Demirdağ T, Aykur M, Günsoy Kiliç Y, Güdeloğlu E, et al. 12-year-old boy with fever, headache and vomiting. Pediatr Infect Dis J. 2024;43:88–90. DOIPubMedGoogle Scholar
- Qvarnstrom Y, Visvesvara GS, Sriram R, da Silva AJ. Multiplex real-time PCR assay for simultaneous detection of Acanthamoeba spp., Balamuthia mandrillaris, and Naegleria fowleri. J Clin Microbiol. 2006;44:3589–95. DOIPubMedGoogle Scholar
- Peng L, Zhou Q, Wu Y, Cao X, Lv Z, Su M, et al. A patient with granulomatous amoebic encephalitis caused by Balamuthia mandrillaris survived with two excisions and medication. BMC Infect Dis. 2022;22:54. DOIPubMedGoogle Scholar
- Cuoco JA, Klein BJ, LeBel DP, Faulhaber J, Apfel LS, Witcher MR. Successful treatment of a Balamuthia mandrillaris cerebral abscess in a pediatric patient with complete surgical resection and antimicrobial therapy. Pediatr Infect Dis J. 2022;41:e54–7. DOIPubMedGoogle Scholar
- Doyle JS, Campbell E, Fuller A, Spelman DW, Cameron R, Malham G, et al. Balamuthia mandrillaris brain abscess successfully treated with complete surgical excision and prolonged combination antimicrobial therapy. J Neurosurg. 2011;114:458–62. DOIPubMedGoogle Scholar
- Botterill E, Yip G. A rare survivor of Balamuthia granulomatous encephalitis. Clin Neurol Neurosurg. 2011;113:499–502. DOIPubMedGoogle Scholar
- Mei J, Sheng F, Zhang C, Chen X. Corrigendum to “Imaging monitoring of Balamuthia granulomatous amoebic encephalitis”. Clin Neurol Neurosurg. 2025;256:
109015 . DOIPubMedGoogle Scholar - Guarner J, Bartlett J, Shieh WJ, Paddock CD, Visvesvara GS, Zaki SR. Histopathologic spectrum and immunohistochemical diagnosis of amebic meningoencephalitis. Mod Pathol. 2007;20:1230–7. DOIPubMedGoogle Scholar
- Dubey P, Kobpornchai P, Tongkrajang N, Chaiyaloom S, Lu C, Rice CA, et al. Drug susceptibility of a clinical isolate of Balamuthia mandrillaris, a pathogenic free-living amoeba. Antimicrob Agents Chemother. 2026;70:
e0148225 . DOIPubMedGoogle Scholar - Aboubechara JP, Kantamneni T, Pasao K. Balamuthia Mandrillaris central nervous system vasculitis in an immunocompetent child: case report. J Child Neurol. 2025;40:366–70. DOIPubMedGoogle Scholar
- Degese MF, Prieto MP, Nigro MG, Perazzo J, Pérez Garófalo M, Lemir G, et al. Free-living amoebae infections: case reports identified at a reference parasitology laboratory in Argentina. Acta Parasitol. 2025;70:240. DOIPubMedGoogle Scholar
- Deetz TR, Sawyer MH, Billman G, Schuster FL, Visvesvara GS. Successful treatment of Balamuthia amoebic encephalitis: presentation of 2 cases. Clin Infect Dis. 2003;37:1304–12. DOIPubMedGoogle Scholar
- Schuster FL, Yagi S, Gavali S, Michelson D, Raghavan R, Blomquist I, et al. Under the radar: Balamuthia amebic encephalitis. Clin Infect Dis. 2009;48:879–87. DOIPubMedGoogle Scholar
- Cary LC, Maul E, Potter C, Wong P, Nelson PT, Given CII, et al. Balamuthia mandrillaris meningoencephalitis: survival of a pediatric patient. Pediatrics. 2010;125:e699–703. DOIPubMedGoogle Scholar
- Moriarty P, Burke C, McCrossin D, Campbell R, Cherian S, Shahab MS, et al. Balamuthia mandrillaris encephalitis: survival of a child with severe meningoencephalitis and review of the literature. J Pediatric Infect Dis Soc. 2014;3:e4–9. DOIPubMedGoogle Scholar
- Orozco L, Hanigan W, Khan M, Fratkin J, Lee M. Neurosurgical intervention in the diagnosis and treatment of Balamuthia mandrillaris encephalitis. J Neurosurg. 2011;115:636–40. DOIPubMedGoogle Scholar
- Yang Y, Hu X, Min L, Dong X, Guan Y. Balamuthia mandrillaris–related primary amoebic encephalitis in China diagnosed by next generation sequencing and a review of the literature. Lab Med. 2020;51:e20–6. DOIPubMedGoogle Scholar
- Yi Z, Zhong J, Wu H, Li X, Chen Y, Chen H, et al. Balamuthia mandrillaris encephalitis in a child: case report and literature review. Diagn Microbiol Infect Dis. 2021;100:
115180 . DOIPubMedGoogle Scholar - Hu J, Zhang Y, Yu Y, Yu H, Guo S, Shi D, et al. Encephalomyelitis caused by Balamuthia mandrillaris in a woman with breast cancer: a case report and review of the literature. Front Immunol. 2022;12:
768065 . DOIPubMedGoogle Scholar - American Academy of Pediatrics Committee on Infectious Diseases. Kimberlin DW, Banerjee R, Barnett ED, Lynfield R, Sawyer MH, editors. Red Book: 2024–2027 Report of the Committee on Infectious Diseases. 33rd edition. Elk Grove Village (IL): American Academy of Pediatrics; 2024.
Figures
Table
Cite This ArticleOriginal Publication Date: June 23, 2026
1These authors contributed equally to this article.
Table of Contents – Volume 32, Number 7—July 2026
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Natasha W. Hanners, University of Texas Southwestern Medical Center, 5323 Harry Hines Blvd, Dallas, TX 75390, USA
Top