Volume 28, Number 2—February 2022
Research Letter
Dirofilaria immitis Pulmonary Dirofilariasis, Slovakia
Cite This Article
Citation for Media
Abstract
Dirofilaria immitis is a parasite related to pulmonary dirofilariasis in humans, its accidental hosts. We detected an autochthonous case of D. immitis infection in a woman from Slovakia. The emergence and spread of this parasite in Europe indicates a critical need for proper diagnosis of infection.
Dirofilaria immitis is a filarioid nematode that infects numerous mammalian species. Dogs are the main reservoir and various mosquito species (e.g., genera Culex, Anopheles, Aedes, and Ochlerotatus) the infection vectors. The parasite is related to the pulmonary form of dirofilariasis, manifested by the formation of coin lesions or nodules in lung parenchyma in humans, an accidental parasite host (1).
In Europe, the species D. repens causes most reported cases of human dirofilariasis. Just over 30 cases of human D. immitis infection have been unambiguously diagnosed, compared with >4,000 from D. repens (2).
In Slovakia, human autochthonous dirofilariasis has occurred since 2007. Meanwhile, 24 cases have been confirmed, all caused by D. repens nematodes (3,4; M. Miterpáková, unpub. data).
In January 2020, a 66-year-old woman from southwestern Slovakia was admitted to the Ambulance of Pneumology and Phthisiology reporting chest pain, cough, and asphyxia. The patient, who had a long-term history of smoking, had been treated for bronchial asthma and chronic obstructive pulmonary disease since 2012. She had not been abroad for >5 years. Results of hematologic and biochemical examinations were within the physiologic ranges; pulmonary function tests revealed moderate obstructive pulmonary disorder: a decrease of vital capacity to 77% (reference range >80%) and forced expiratory volume during the first second to 63% (reference range >80%). A chest radiograph showed bilaterally hyperlucent lungs with coarse bronchovascular markings; therefore, emphysema was suspected. Subsequent computed tomography confirmed bilateral paraseptal emphysema and numerous nonspecific lesions, ≈5 mm in diameter, in the S2 segment of the right lung and solitary nodules in the S8/9 segment of the left lung. Because of suspected malignancy, the patient was regularly monitored. After 12 months, the cancer markers had elevated. A control computed tomography examination showed a subpleural focal lesion in the S10 segment of the right lung; positron emission tomography/computed tomography confirmed hypermetabolic activity of the lesion. Biopsy was recommended because of a suspected tumor.
Figure
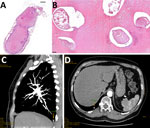
Figure. Histologic examination of resected tissue from a 66-year-old woman from southwestern Slovakia. A, B) Cross section showing Dirofilaria immitisnematodes embedded in necrotic material obtained from well-defined pulmonary nodule....
In May 2021, a wedge surgical resection of the nodule was performed. Histologic examination of resected tissue revealed a well-circumscribed necrotic nodule containing small irregularly shaped tubular formations affected by massive degenerative changes. The edge of the nodule consisted of nonspecific fibrotic and inflammatory granulations (Figure). The final pathology report suggested the presence of massively degenerated fragments of a nonvital parasite, with Dirofilaria spp. suspected.
We amplified the mitochondrial cox1 gene fragments of D. repens (209 bp) and D. immitis (203 bp), in accordance with Rishniw et al. (5). The analyzed tissue was positive for D. immitis and subsequent sequencing and BLAST analysis of the sequence (GenBank accession no. MZ438680) revealed 100% identity within the region overlapping other homologous D. immitis sequences from GenBank (e.g., accession nos. KC985239, NC005305).
Pulmonary dirofilariasis is still very rare in Europe, and many cases are evaluated as imported. Even cases published as autochthonous are still under discussion, and no final decision has been reached. For instance, Pampiglione et al. (6) published an analysis of 28 human cases diagnosed in Europe and attributed to D. immitis parasites or a species other than D. repens. In this analysis the researchers excluded D. immitis parasites as a causative agent in all the reviewed cases (6). A nonspecific localization of D. repens infection in lung tissue was recently reported in several patients from Russia, and 1 case was diagnosed in Slovakia (3,7). Recent data from several European countries, including Slovakia, indicate dramatic increase of D. immitis infections in the canine population (4,8,9), which may cause a rise in human cases in the near future.
Human pulmonary dirofilariasis is characterized by the formation of typical nodules (coin lesions) around immature adult worms located mainly on the lung periphery (6). Differential diagnosis of the nodules is important because >20 other pathologic conditions manifests by coin lesions, including tumors, cysts, and inflammatory granulomas. Coin lesions observed in patients with pulmonary dirofilariasis are spherical, not pyramidal as embolic infarct, and generally range from 1 cm to 4.5 cm in diameter (10). Few patients with pulmonary dirofilariasis show clinical symptoms. When symptoms are present, they are nonspecific and include thoracic pain, cough, and purulent sputum. These symptoms imitate pneumonitis, and patients are often treated incorrectly with antimicrobial drugs (1).
Long-term experience from dirofilariasis-endemic areas confirms that diagnosis is key and still a great challenge in the successful encompassment of human pulmonary dirofilariasis. Given the lack of specific and sensitive serologic tests, the only way for correct presurgical diagnosis appears to be the use of medical imaging. According to the European Society of Dirofilariosis and Angiostrongylosis (2), the combination of ultrasound and color Doppler charting, which offers findings of well-defined characteristics of D. immitis nodules (e.g., regular oval shape, hypoechoic inner content, no signs of polar vascularity) enable attribution to helminthic origin.
Dr. Miterpáková is a senior researcher and deputy director at the Institute of Parasitology of the Slovak Academy of Sciences in Košice, Slovakia. Her primary research interests include epidemiology, ecology and diagnosis of parasitic diseases; zoonoses; and vectorborne diseases.
Acknowledgments
The study was supported by the Science Grant Agency, VEGA project no. 2/0014/21 and by the Slovak Research and Development Agency under the contract no. APVV-15-0114.
The patient agreed with all examinations and publication of case report and signed the informed content. No identifying data are presented in the paper. The study was performed in accordance with the ethical standards as laid down in the Declaration of Helsinki of 1975, as revised 2013.
References
- Simón F, Siles-Lucas M, Morchón R, González-Miguel J, Mellado I, Carretón E, et al. Human and animal dirofilariasis: the emergence of a zoonotic mosaic. Clin Microbiol Rev. 2012;25:507–44. DOIPubMedGoogle Scholar
- European Society of Dirofilariosis and Angiostrongylosis. Guidelines for clinical management of human Dirofilaria infections. 2017 [cited 2021 Jul 28]. https://www.esda.vet/wp-content/uploads/2017/11/Guidelines-For-Clinical-Management-Of-Human-Dirofilaria-Infections.pdf
- Miterpáková M, Antolová D, Ondriska F, Gál V. Human Dirofilaria repens infections diagnosed in Slovakia in the last 10 years (2007-2017). Wien Klin Wochenschr. 2017;129:634–41. DOIPubMedGoogle Scholar
- Fuehrer HP, Morelli S, Unterköfler MS, Bajer A, Bakran-Lebl K, Dwużnik-Szarek D, et al. Dirofilaria spp. and Angiostrongylus vasorum: current risk of spreading in Central and Northern Europe. Pathogens. 2021;10:1268. DOIPubMedGoogle Scholar
- Rishniw M, Barr SC, Simpson KW, Frongillo MF, Franz M, Dominguez Alpizar JL. Discrimination between six species of canine microfilariae by a single polymerase chain reaction. Vet Parasitol. 2006;135:303–14. DOIPubMedGoogle Scholar
- Pampiglione S, Rivasi F, Gustinelli A. Dirofilarial human cases in the Old World, attributed to Dirofilaria immitis: a critical analysis. Histopathology. 2009;54:192–204. DOIPubMedGoogle Scholar
- Moskvina T, Ermolenko AV. Dirofilariasis in Russian Federation: a big problem with large distribution. Russian Open Medical Journal. 2018;7:
e0102 . DOIGoogle Scholar - Széll Z, Bacsadi Á, Szeredi L, Nemes C, Fézer B, Bakcsa E, et al. Rapid spread and emergence of heartworm resulting from climate and climate-driven ecological changes in Hungary. Vet Parasitol. 2020;280:
109067 . DOIPubMedGoogle Scholar - Miterpáková M, Hurníková Z, Valentová D, Borková L. Different epidemiological pattern of canine dirofilariosis in two neighboring countries in Central Europe-the Czech Republic and Slovakia. Parasitol Res. 2021;120:547–52. DOIPubMedGoogle Scholar
- Seybold WD. Solitary or “coin” lesions of the lung. Postgrad Med. 1964;36:424–30. DOIPubMedGoogle Scholar
Figure
Cite This ArticleOriginal Publication Date: January 13, 2022
Table of Contents – Volume 28, Number 2—February 2022
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Daniela Antolová, Institute of Parasitology SAS, Hlinkova 3, 040 01 Košice, Slovakia
Top