Volume 32, Number 3—March 2026
Research
Projected Effects of Changing Global Tuberculosis Epidemiology on Mycobacterium tuberculosis Immunoreactivity Prevalence, 2024–2050
Cite This Article
Citation for Media
Abstract
We assessed how evolving global tuberculosis (TB) trends might influence Mycobacterium tuberculosis immunoreactivity and TB risk among persons immigrating to low-incidence countries. We projected annual risk for infection (ARI) in 168 countries for 2024–2050, focusing on China, India, the Philippines, and Vietnam. We applied projections to the age profile of immigrants to 4 low-incidence countries to estimate changes in M. tuberculosis immunoreactivity prevalence and TB risk under status quo and accelerated ARI decline scenarios. In the status quo 2024 estimate, M. tuberculosis immunoreactivity prevalence ranged from 14.7% in China to 40.1% in the Philippines, declining to 5.8% in China and 23.0% in the Philippines by 2050; TB risk also declined. Accelerated ARI reductions yielded greater relative decreases in disease risk than immunoreactivity prevalence. Declining global TB incidence could reduce M. tuberculosis immunoreactivity and disease risk among immigrant populations, which could inform cost–benefit analyses for future TB screening strategies in low-incidence settings.
Tuberculosis (TB) remains a major global public health challenge. In 2024, an estimated 10.7 million persons had TB develop, and ≈1.23 million persons died (1). TB, caused by Mycobacterium tuberculosis, begins as an asymptomatic infection but can progress to infectious disease at any time (2). Among persons with evidence of M. tuberculosis infection, risk of developing TB is highest in the first 2 years after infection (3). Persons with evidence of M. tuberculosis infection go through a short high-risk period, followed by a prolonged low-risk period (1–3).
M. tuberculosis infection is diagnosed by absence of clinical findings indicating TB disease, plus immunoreactivity to M. tuberculosis antigens measured by skin tests or interferon-γ release assays (4,5). Immunoreactivity can exhibit reversion (6) but is assumed to be lifelong for many infected persons. Immunoreactivity tests cannot distinguish persons at high risk for TB progression (i.e., recently infected [<2 years]) from those at low risk (i.e., remotely infected [>2 years]). The number of recently infected versus remotely infected persons will vary by local epidemiology, driven by the force of M. tuberculosis transmission.
In many low-incidence countries, TB disproportionately affects immigrant populations, largely because of progression of M. tuberculosis infection acquired in higher transmission settings before immigration. For that reason, several countries have implemented or considered large-scale M. tuberculosis infection screening and treatment programs among new immigrants (7,8). Critical to the cost-effectiveness of those programs are M. tuberculosis immunoreactivity prevalence and the likelihood of subsequent TB disease (9). TB risk is directly correlated with the percentage of recently infected persons; thus, understanding how changing TB epidemiology affects immunoreactivity prevalence and percentages of persons recently or remotely infected can have implications for cost-effectiveness and efficiency of TB programs.
In this study, we aimed to gain insights into how changing TB epidemiology would affect the M. tuberculosis immunoreactivity prevalence and risk for developing TB disease among new immigrants to low-incidence countries. Using the age distribution of new immigrants to 4 immigrant-receiving low-incidence countries, we estimated temporal changes in the overall M. tuberculosis immunoreactivity prevalence and risk for progression to TB disease in the year of arrival among immigrants from 168 countries. We focused on immigrants from 4 moderate- to high-incidence countries, India, China, the Philippines, and Vietnam, and modeled how further changes in M. tuberculosis transmission could affect those outcomes for 2024–2050.
Countries Evaluated
For this analysis, we considered persons immigrating from 168 countries (Appendix Table 1). Of those, we selected 4 moderate- to high-incidence countries (annual TB incidence ≥50/100,000 population) to examine more closely: China, India, the Philippines, and Vietnam. We selected those countries because all 4 are common countries of origin for immigrants moving to 4 common immigrant-receiving countries. In 2023, those 4 countries combined accounted for 54% of new immigrants to Canada, 19% to the United States, 12% to the United Kingdom, and 47% to Australia (10–13).
Annual Risk for M. tuberculosis Infection Measured by Immunoreactivity
The diagnosis of M. tuberculosis infection is based on immunoreactivity to skin tests or interferon-γ release assays and cannot be empirically confirmed; thus, we focused on immunoreactivity. We estimated the annual risk for infection (ARI), which is the probability that in a given year someone will become M. tuberculosis immunoreactive, by leveraging methods and estimates generated for a previously published analysis (14). Estimates included 200 different ARI projections from 1889–2021. When available, we used historical tuberculin skin test surveys as the basis for ARI; in all other instances, we estimated ARI by using a modified Styblo rule, which relates the prevalence of smear-positive TB disease to the ARI. In both methods, ARI is related to measured immunoreactivity prevalence, and immunoreactivity is assumed to be lifelong. To estimate ARI beyond 2021, we estimated the average annual change in ARI during 2000–2021 and projected the same annual change from 2022 to 2050 for each country and ARI projection.
Estimation of M. tuberculosis Immunoreactivity Prevalence
To estimate M. tuberculosis immunoreactivity prevalence, we adapted methods from a previously published study modeling immunoreactivity prevalence among foreign-born residents of Canada (14). In brief, we calculated the cumulative probability of M. tuberculosis immunoreactivity by integrating the ARI over time stratified by country of origin, year of birth, and year of migration. We applied annual ARI values sequentially up to each time point, assuming independent infection risk from year to year.
For each country, we used the 200 ARI trajectories estimated for 2024 to 2050 to generate 200 corresponding estimates of immunoreactivity prevalence for each year of migration and year of birth. We then applied those estimates to the age distribution of new immigrants from 4 immigrant-receiving low-incidence countries, to attain estimates of overall immunoreactivity prevalence for each year. Similarly, we used those same ARI trajectories to estimate the prevalence of recently acquired M. tuberculosis immunoreactivity (i.e., persons who became immunoreactive <2 years), using the ARI over a 2-year period. We selected a 2-year period for recent immunoreactivity because that timeframe corresponds to the highest risk period for progression to TB (3,5,15).
Projections of M. tuberculosis Immunoreactivity Prevalence and TB Risk
To estimate the age distribution of immigrants, we analyzed immigration data from Canada, the United States, the United Kingdom, and Australia, which detail the demographic characteristics of new immigrants each year (Appendix). We categorized those values into 6 age ranges: 0–14, 15–29, 30–44, 45–59, 60–74, and >75 years (16). We assumed the age distribution was the same for each country of origin and that specific ages were equally distributed within each range.
To project the age distribution into the future, we calculated the mean percentage and SD of new immigrants belonging to each age group in the most recent year from which data were available (2023–2024) across countries by using equal weighting and assumed that distribution remained stable from 2024 to 2050. We fit each age category to a β distribution (Appendix Table 2), and generated 200 sets of age distribution estimates, scaling values to ensure each set summed to 100%. Therefore, we estimated that, of all new immigrants, 16.4% (95% uncertainty interval [UI] 10.3%–24.9%) would be 0–14 years of age, 25.2% (95% UI 14.4%–36.8%) would be 15–29 years of age, 34.5% (95% UI 24.4%–47.0%) would be 30–44 years of age, 15.3% (95% UI 8.5%–24.8%) would be 45–59 years of age, 6.3% (95% UI 2.7%–11.4%) would be 60–74 years of age, and 1% (95% UI 0.3%–2.5%) would be ≥75 years of age at the time of immigration.
For each year during 2024–2050, we used each of the 200 ARI trajectories to estimate the overall M. tuberculosis immunoreactivity prevalence among persons immigrating from each country, as well as the acquired immunoreactivity prevalence in the previous 2 years under a status quo scenario (i.e., no change in projected ARI trajectories). Using the projections of overall and recent M. tuberculosis immunoreactivity, we estimated the average annual TB incidence in the year of arrival among new immigrants overall from each country, as well as the TB incidence in the year of arrival restricted to those with underlying M. tuberculosis immunoreactivity.
To estimate risk for TB progression, we assumed that the annual risk for TB progression for persons who recently acquired immunoreactivity was similar to that estimated in a large systematic review of TB risk among contacts (17). For persons with remotely (>2 years before immigration) acquired immunoreactivity, we based estimates on observed TB incidence data in Canada (Appendix). We used those data sources to fit risks to lognormal distributions (Appendix) and generated 200 estimates, which resulted in estimates of TB risk in the year of arrival at 1.7% (95% UI 1.3%–2.2%) among persons with recent M. tuberculosis immunoreactivity and at 0.07% (95% UI 0.06%–0.09%) among persons with remote M. tuberculosis immunoreactivity.
To assess how reducing M. tuberculosis transmission would affect each of those outcomes, we modeled 3 different scenarios in which we reduced the ARI trajectories in our status quo projections beginning in 2025 to an absolute 1% additional reduction, 3% additional reduction, and 5% additional reduction in ARI. For example, if the status quo scenario had an estimated annual relative ARI decrease of 3% for a given country, we modeled scenarios in which the relative ARI decrease was 4%, 6%, or 8% annually. We calculated absolute and relative reductions by comparing each reduction scenario to the status quo. We stratified data by country and by age groups to identify trends and differences in estimates among strata.
We conducted a sensitivity analysis in which we loosened our assumption that M. tuberculosis immunoreactivity was lifelong, allowing for reversion (6,18). Because our ARI estimates are based on measured immunoreactivity, if reversion occurred, we would estimate the same level of overall measured immunoreactivity prevalence, but ARI would necessarily need to be higher to achieve that prevalence. Using those higher ARIs, recently acquired immunoreactivity prevalence would increase. Therefore, to maintain observed levels of immunoreactivity in our sensitivity analysis, we estimated the attendant increase in the ARI assuming an annual reversion rate of 10%, per previously described data (18,19). Thus, considering reversion was equivalent to a 2.9-fold increase in ARI, and we used that assumption to reestimate the prevalence of recently acquired immunoreactivity and the average annual risk for TB progression for the years 2024–2050.
We reported estimates as medians and 95% UIs (2.5th and 97.5th percentiles) across the 200 ARI trajectories. We compared outputs of M. tuberculosis immunoreactivity prevalence and TB disease risk to previous estimates for face validity (Appendix). We conducted all analyses in R version 4.3.1 (The R Project for Statistical Computing, https://www.r-project.org). We performed preliminary data organization and cleaning using Excel 2024 (Microsoft, https://www.microsoft.com). We created graphic representations using the ggplot2 package version 3.5.1 (https://github.com/cran/ggplot2) and GraphPad (GraphPad Software Inc., https://www.graphpad.com). This study used publicly available deidentified, aggregate data, and did not include personal identifiers in any data analyzed; thus, approval from a research ethics board was not required.
Estimated Changes in ARI
We estimated the Philippines would have the highest 2024 ARI at 0.98% (95% UI 0.46%–2.2%), followed by India at 0.48% (95% UI 0.24%–0.95%), Vietnam at 0.41% (95% UI 0.13%–1.20%), and China at 0.19% (95% UI 0.08%–0.47%) (Table 1; Appendix Figure 1). Across all 4 countries, the estimated ARI generally declined during 2000–2021, although in all countries except India, a small number of trajectories projected increases. Specifically, we estimated the ARI would fall at a relative rate of 3.8% per year (95% UI 7.3% decline to 0.2% increase) in China, 4.1% per year (95% UI 7.1% decline to 0.2% decline) in India, 3.1% per year (95% UI 7.1% decline to 0.7% increase) in the Philippines, and 3.8% per year (95% UI 8.8% decline to 1.6% increase) in Vietnam. Following those projections, compared with 2024, the 2050 ARI was 61.8% lower (95% UI 84.7% lower to 5.0% higher) in China, 64.7% lower (95% UI 84.0% lower to 5.5% higher) in India, 53.8% lower (95% UI 83.9% lower to 19.5% higher) in the Philippines, and 61.6% lower (95% UI 89.7% lower to 46.8% higher) in Vietnam. We also calculated ARI trends for all 168 countries (Appendix Table 3).
Projected Changes in Immunoreactivity Prevalence
Figure 1

Figure 1. Projected immunoreactivity in study of effects of global tuberculosis epidemiology on Mycobacterium tuberculosis immunoreactivity prevalence, 2024–2050. Graphs show projected prevalence of M. tuberculosisimmunoreactivity among immigrants from...
In general, declining ARI trends translated into reductions in the point estimates of immunoreactivity prevalence among immigrant populations from China, India, the Philippines, and Vietnam. In 2024, we estimated prevalence among new immigrants from each country to be 14.7% (95% UI 10.7%–22.7%) for China, 25.4% (95% UI 20.4%–30.8%) for India, 40.1% (95% UI 32.6%–49.8%) for the Philippines, and 27.7% (95% UI 19.5%–41.2%) for Vietnam (Figure 1). By 2050, we projected prevalence would decrease to 5.8% (95% UI 3.4%–13.5%) for China, 13.2% (95% UI 7.7%–26.2%) for India, 23.0% (95% UI 14.3%–48.5%) for the Philippines, and 11.7% (95% UI 6.9%–30.5%) for Vietnam (Appendix Tables 4, 5).
The prevalence of recent immunoreactivity remained relatively stable over time in the status quo scenario. By 2050, we projected the prevalence of recently acquired immunoreactivity would be 0.14% (95% UI 0.03%–0.78%) for China, 0.30% (95% UI 0.07%–1.40%) for India, 0.67% (95% UI 0.14%–2.6%) for the Philippines, and 0.28% (95% UI 0.03%–2.1%) for Vietnam (Appendix Table 6). In our reversion sensitivity analysis, corresponding estimates in 2050 were 0.4% (95% UI 0.08%–2.3%) for China, 0.86% (95% UI 0.21%–4.1%) for India, 1.9% (95% UI 0.41%–7.4%) for the Philippines, and 0.80% (95% UI 0.08%–6.0%) for Vietnam (Appendix Table 6).
Figure 2
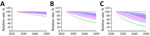
Figure 2. Projected effects on tuberculosis (TB) incidence and Mycobacterium tuberculosis immunoreactivity in study of effects of global tuberculosis epidemiology on M. tuberculosisimmunoreactivity prevalence, 2024–2050. Graphs show effects...
Figure 3
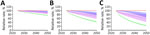
Figure 3. Projected effects on tuberculosis (TB) incidence and Mycobacterium tuberculosis immunoreactivity in study of effects of global tuberculosis epidemiology on M. tuberculosisimmunoreactivity prevalence, 2024–2050. Graphs show effects...
Figure 4
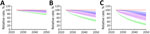
Figure 4. Projected effects on tuberculosis (TB) incidence and Mycobacterium tuberculosis immunoreactivity in study of effects of global tuberculosis epidemiology on M. tuberculosisimmunoreactivity prevalence, 2024–2050. Graphs show effects...
Figure 5
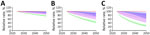
Figure 5. Projected effects on tuberculosis (TB) incidence and Mycobacterium tuberculosis immunoreactivity in study of effects of global tuberculosis epidemiology on M. tuberculosisimmunoreactivity prevalence, 2024–2050. Graphs show effects...
Increasing the rate of ARI decline had modest effects on the absolute decline in immunoreactivity prevalence, regardless of the increase in the rate of decline (Appendix Tables 7, 8). We noted much greater effects on the prevalence of recent M. tuberculosis immunoreactivity under ARI decline scenarios (Figures 2,3,4,5). Under the additional 1% ARI decline scenario, we projected the overall immunoreactivity prevalence across China, India, the Philippines, and Vietnam would decrease by ≈6% by 2050 relative to the status quo scenario. However, recent immunoreactivity prevalence fell more sharply, declining by ≈25%. Under the additional 5% ARI decline scenario, those reductions were more pronounced; overall immunoreactivity prevalence decreased by up to 21%–23%, and recent immunoreactivity prevalence fell by 75%–77% relative to the status quo.
Age-stratified projections revealed that declines in immunoreactivity prevalence varied by age group and had a strong inverse relationship between age and reduction magnitude. Younger cohorts, having experienced fewer cumulative years of exposure, received the largest benefits from reduced ARI. For instance, by 2050 under the additional 3% ARI decline scenario, we projected the immunoreactivity in children 0–14 years of age would fall below 1% among children from China, India, and Vietnam, although it remained slightly above 1% for children from the Philippines. In contrast, older adults retained higher immunoreactivity levels due to prior exposures accumulated over their lifetimes (Appendix Table 9). The most substantial declines occurred in settings with initially high transmission, notably the Philippines and India, where the effects of accelerated ARI reductions were substantial. As expected, the percentage of recently acquired immunoreactivity was highest in the youngest age groups and increased in sensitivity analyses that incorporated reversion (Appendix Tables 10, 11).
Projected Changes in the Average TB Risk
Under the status quo scenario, we estimated overall annual TB incidence per 100,000 new immigrants arriving in 2024 would be 16.4 (95% UI 11.0–24.9) among those from China, 29.7 (95% UI 20.1–47.4) among those from India, 47.9 (95% UI 34.5–72.0) among those from the Philippines, and 30.2 (95% UI 21.2–47.3) among those from Vietnam. We projected that by 2050 those risks among new immigrants would fall to 6.4 (95% UI 3.0–22.7) among those from China, 14.5 (95% UI 6.8–41.9) among those from India, 27.1 (95% UI 12.2–76.0) among those from the Philippines, and 12.9 (95% UI 5.9–53.9) among those from Vietnam (Table 2; Appendix Table 12). As a result of the higher estimated prevalence of recently acquired immunoreactivity, we estimated TB incidence in the arrival year would be nearly double in sensitivity analyses incorporating immunoreactivity reversion (Table 2; Appendix Tables 13, 14).
Accelerating declines in ARI led to further reductions in TB risk, largely driven by reductions in the prevalence of recently acquired M. tuberculosis immunoreactivity (Appendix Figure 2). Under the additional 3% ARI decline scenario, we estimated the annual risk per 100,000 new immigrants arriving in 2050 would be 4.4 (95% UI 2.3–12.7) among those from China, 10.1 (95% UI 5.4–24.2) among those from India, 18.5 (95% UI 9.0–48.7) among those from the Philippines, and 9.1 (95% UI 5.0–32.8) among those from Vietnam (Table 2). As with immunoreactivity prevalence, we noted greater declines in TB risk in younger age categories (Appendix Tables 12, 13). When we estimated TB risk in arrival year only among those with M. tuberculosis immunoreactivity, TB risk fell by ≈7% in the additional 1% ARI decline scenario, 18% in the 3% scenario, and 25% in the 5% scenario relative to the status quo (Appendix Table 15).
In this study, we found that among 4 countries with moderate to high TB incidence, China, India, the Philippines, and Vietnam, recent trends suggest ARI is falling 2%–3% per year. Accordingly, we projected M. tuberculosis immunoreactivity prevalence, a proxy for M. tuberculosis infection, and average TB risk would decrease among immigrants from those countries by 2050, and the Philippines would have the greatest absolute declines. Accelerating ARI declines, even by modest amounts, had larger relative effects on TB risks compared with M. tuberculosis immunoreactivity prevalence, primarily driven by declines in recently acquired immunoreactivity.
The cost-effectiveness of immigration M. tuberculosis infection screening and treatment programs is an ongoing area of debate. Some analyses have found such programs to be highly cost-prohibitive (20–22), but others have found them to be cost-effective compared with traditionally accepted willingness-to-pay thresholds (23,24). However, the major drivers of the cost effectiveness of any M. tuberculosis infection screening program are the underlying prevalence of M. tuberculosis immunoreactivity and risk of developing TB. Our analysis projects the cost effectiveness of those programs to generally worsen over time as the immunoreactivity prevalence and risk of developing TB decline. For instance, our estimates showed that, among new immigrants from the Philippines, immunoreactivity prevalence would drop from 40.1% in 2024 to 23.0% in 2050 and TB risk in the year of arrival would fall from 47.9/100,000 immigrants in 2024 to 27.1/100,000 immigrants in 2050. However, those effects are unlikely to be homogenous within and between countries. That finding highlights the need for constant evaluation of TB screening programs where they are implemented (25) to ensure efficient use of healthcare funds.
A 2024 modeling study highlighted the potential economic and health benefits of improvements in global TB prevention and care in low-incidence settings (26). In line with those findings, we found substantial reductions in the population-level TB risk in scenarios with accelerated ARI declines. We also found that in those scenarios, TB risk declined more rapidly than overall M. tuberculosis immunoreactivity prevalence. That finding suggests that, in addition to the overall decline in population-level TB risk, the individual-level risk–benefit calculus of providing TB preventive treatment could change. Therefore, if declines in global TB incidence accelerate in the future, programs would need to anticipate and adapt to those changes, such as by using more targeted approaches to TB screening and treatment.
We found consideration of M. tuberculosis immunoreactivity reversion increased estimates of TB disease risks in the year of arrival for new immigrants, driven by higher ARIs and therefore increased prevalence of recently acquired M. tuberculosis immunoreactivity. That aspect has been identified by others (27). However, cohort data have shown TB risk persists, albeit reduced, among persons who had immunoreactivity reversion, and that reversion might not be stable (i.e., persons reconvert to immunopositive) (6). The extent of stable immunoreactivity reversion thus has implications on the value of prompt immunoreactivity testing and treatment after immigration (28), when risk for recent exposure would be highest.
Key strengths of this study are the consideration of multiple policy-relevant outcomes, use of previously reported data and methodology to perform the analyses, and consistency of our estimates with existing empiric literature. In addition, we included a breadth of countries and focused on countries comprising a large number of new immigrants to low-incidence countries. We also used uncertainty in several key underlying parameters and explored the effects of underlying assumptions around immunoreactivity reversion.
The first limitation of our study is that our analysis equated M. tuberculosis immunoreactivity to infection. Because current technologies to identify M. tuberculosis infection rely on immunoreactivity and data underlying TB progression rates reflect observations based on immunoreactivity, that was a reasonable approach. However, our main analysis assumed M. tuberculosis immunoreactivity would be lifelong, which might underestimate prevalence of recently acquired immunoreactivity. Therefore, we evaluated the effect of that assumption in a sensitivity analysis. When we incorporated immunoreactivity reversion, which implies a higher estimated prevalence of recently acquired immunoreactivity, the estimated TB risks increased. Second, we made several simplifying assumptions to focus the analysis on the potential effect of changing infection risks. We projected ARI trends beyond 2021 on the basis of trends from 2000–2021 and used a similar age distribution for immigrants from all countries. Those assumptions might not hold true for all countries if immigration patterns change or if global TB funding is interrupted (1,29). Third, we did not consider protection from reinfection in our model (30), which might lead to slight overestimation of the percentage of persons with recent infection. Fourth, we assumed no heterogeneity in risk for M. tuberculosis immunoreactivity or TB progression by demographic, clinical, or other factors among immigrants from each country. We did not explicitly model specific high-risk groups (e.g., persons with HIV) within immigrant cohorts and did not consider immigrants to differ systematically from nonimmigrants within any given country when considering infection or TB progression.
In summary, we found changing global TB epidemiology could lead to reduced M. tuberculosis immunoreactivity and TB risk among immigrants to low-incidence countries. Such changes might worsen the cost-effectiveness of M. tuberculosis infection screening and treatment programs, requiring further targeting of these programs over time, as well as alter the individual-level balance of risks and benefits of TB preventive treatment.
Ms. Machado works in health economics and outcomes research McGill University, Montreal, Quebec, Canada. Her research interests focus on generating evidence to support health equity and access to care, particularly among vulnerable populations.
Author contributions: J.R.C. and K.S. initially conceptualized the study; M.M., A.E.J., and J.R.C. conducted analysis; M.M. and J.R.C. wrote the first draft; and all authors contributed to study development and interpretation and revised the final draft. All authors meet ICMJE criteria for authorship and have seen and approved the final submitted version.
Acknowledgments
All code and data underlying the analysis are available at https://github.com/michelle-machado/TB-immigrants-risk-projection/tree/main.
This work was funded by the Canadian Institutes of Health Research (grant nos. PJT-190227 and PJT-173348).
J.R.C. receives salary support from the McGill University Health Centre Foundation and the McGill University Department of Medicine and holds a Chercheur-boursier award from the Fonds de recherche du Québec—Santé (no. 330287 https://doi.org/10.69777/330287).
References
- World Health Organization. Global tuberculosis report 2025. Geneva: The Organization; 2025.
- Trajman A, Campbell JR, Kunor T, Ruslami R, Amanullah F, Behr MA, et al. Tuberculosis. Lancet. 2025;405:850–66. DOIPubMedGoogle Scholar
- Getahun H, Matteelli A, Abubakar I, Aziz MA, Baddeley A, Barreira D, et al. Management of latent Mycobacterium tuberculosis infection: WHO guidelines for low tuberculosis burden countries. Eur Respir J. 2015;46:1563–76. DOIPubMedGoogle Scholar
- Gupta RK, Calderwood CJ, Yavlinsky A, Krutikov M, Quartagno M, Aichelburg MC, et al. Discovery and validation of a personalized risk predictor for incident tuberculosis in low transmission settings. Nat Med. 2020;26:1941–9. DOIPubMedGoogle Scholar
- Houben RMGJ, Dodd PJ. The global burden of latent tuberculosis infection: a re-estimation using mathematical modelling. PLoS Med. 2016;13:
e1002152 . DOIPubMedGoogle Scholar - Dale KD, Schwalb A, Coussens AK, Gibney KB, Abboud AJ, Watts K, et al. Overlooked, dismissed, and downplayed: reversion of Mycobacterium tuberculosis immunoreactivity. Eur Respir Rev. 2024;33:
240007 . DOIPubMedGoogle Scholar - Kunst H, Burman M, Arnesen TM, Fiebig L, Hergens MP, Kalkouni O, et al. Tuberculosis and latent tuberculous infection screening of migrants in Europe: comparative analysis of policies, surveillance systems and results. Int J Tuberc Lung Dis. 2017;21:840–51. DOIPubMedGoogle Scholar
- Pareek M, Baussano I, Abubakar I, Dye C, Lalvani A. Evaluation of immigrant tuberculosis screening in industrialized countries. Emerg Infect Dis. 2012;18:1422–9. DOIPubMedGoogle Scholar
- Mahon J, Beale S, Holmes H, Arber M, Nikolayevskyy V, Alagna R, et al. A systematic review of cost-utility analyses of screening methods in latent tuberculosis infection in high-risk populations. BMC Pulm Med. 2022;22:375. DOIPubMedGoogle Scholar
- Government of Canada. Permanent residents—monthly IRCC updates—Canada—permanent residents by country of citizenship [cited 2025 Apr 25]. https://open.canada.ca/data/en/dataset/f7e5498e-0ad8-4417-85c9-9b8aff9b9eda/resource/d1c1f4f3-2d7f-4e02-9a79-7af98209c2f3
- Ward AUS. lawful permanent residents. Washington: US Department of Homeland Security; 2023.
- GOV.UK. How many people are granted settlement or citizenship? [cited 2025 Apr 25]. https://www.gov.uk/government/statistics/immigration-system-statistics-year-ending-december-2023/how-many-people-are-granted-settlement-or-citizenship
- Australian Government, Department of Home Affairs [cited 2025 Apr 25]. https://www.homeaffairs.gov.au
- Jordan AE, Nsengiyumva NP, Houben RMGJ, Dodd PJ, Dale KD, Trauer JM, et al. The prevalence of tuberculosis infection among foreign-born Canadians: a modelling study. CMAJ. 2023;195:E1651–9. DOIPubMedGoogle Scholar
- Pinto PFPS, Teixeira CSS, Ichihara MY, Rasella D, Nery JS, Sena SOL, et al. Incidence and risk factors of tuberculosis among 420 854 household contacts of patients with tuberculosis in the 100 Million Brazilian Cohort (2004-18): a cohort study. Lancet Infect Dis. 2024;24:46–56. DOIPubMedGoogle Scholar
- Government of Canada. Permanent residents—monthly IRCC updates [cited 2025 May 6]. https://open.canada.ca/data/en/dataset/f7e5498e-0ad8-4417-85c9-9b8aff9b9eda
- Campbell JR, Winters N, Menzies D. Absolute risk of tuberculosis among untreated populations with a positive tuberculin skin test or interferon-gamma release assay result: systematic review and meta-analysis. BMJ. 2020;368:m549. DOIPubMedGoogle Scholar
- Schwalb A, Emery JC, Dale KD, Horton KC, Ugarte-Gil CA, Houben RMGJ. Impact of reversion of Mycobacterium tuberculosis immunoreactivity tests on the estimated annual risk of tuberculosis infection. Am J Epidemiol. 2023;192:1937–43. DOIPubMedGoogle Scholar
- Schwalb A, Dodd PJ, Rickman HM, Ugarte-Gil CA, Horton KC, Houben RMGJ. Estimating the global burden of viable Mycobacterium tuberculosis infection: A mathematical modelling study. PLoS Med. 2026;23:
e1004920 . DOIPubMedGoogle Scholar - Campbell JR, Johnston JC, Sadatsafavi M, Cook VJ, Elwood RK, Marra F. Cost-effectiveness of post-landing latent tuberculosis infection control strategies in new migrants to Canada. PLoS One. 2017;12:
e0186778 . DOIPubMedGoogle Scholar - Dale KD, Abayawardana MJ, McBryde ES, Trauer JM, Carvalho N. Modeling the cost-effectiveness of latent tuberculosis screening and treatment strategies in recent migrants to a low-incidence setting. Am J Epidemiol. 2022;191:255–70. DOIPubMedGoogle Scholar
- Shedrawy J, Deogan C, Öhd JN, Hergens MP, Bruchfeld J, Jonsson J, et al. Cost-effectiveness of the latent tuberculosis screening program for migrants in Stockholm Region. Eur J Health Econ. 2021;22:445–54. DOIPubMedGoogle Scholar
- Linas BP, Wong AY, Freedberg KA, Horsburgh CR Jr. Priorities for screening and treatment of latent tuberculosis infection in the United States. Am J Respir Crit Care Med. 2011;184:590–601. DOIPubMedGoogle Scholar
- Tasillo A, Salomon JA, Trikalinos TA, Horsburgh CR Jr, Marks SM, Linas BP. Cost-effectiveness of testing and treatment for latent tuberculosis infection in residents born outside the United States with and without medical comorbidities in a simulation model. JAMA Intern Med. 2017;177:1755–64. DOIPubMedGoogle Scholar
- Centers for Disease Control and Prevention. Immigrant and refugee health—tuberculosis [cited 2025 May 9]. https://www.cdc.gov/immigrant-refugee-health/hcp/civil-surgeons/tuberculosis.html
- Menzies NA, Swartwood NA, Cohen T, Marks SM, Maloney SA, Chappelle C, et al. The long-term effects of domestic and international tuberculosis service improvements on tuberculosis trends within the USA: a mathematical modelling study. Lancet Public Health. 2024;9:e573–82. DOIPubMedGoogle Scholar
- Dowdy DW, Behr MA. Are we underestimating the annual risk of infection with Mycobacterium tuberculosis in high-burden settings? Lancet Infect Dis. 2022;22:e271–8. DOIPubMedGoogle Scholar
- Greenaway C, Diefenbach-Elstob T, Schwartzman K, Cook VJ, Giovinazzo G, Njoo H, et al. Tuberculosis surveillance and tuberculosis infection testing and treatment in migrants. In: Canadian tuberculosis standards, 8th edition. Menzies D, editor. Montreal: Canadian Thoracic Society; 2022. p. 194–204.
- Clark RA, McQuaid CF, Richards AS, Bakker R, Sumner T, Prŷs-Jones TO, et al. The potential impact of reductions in international donor funding on tuberculosis in low-income and middle-income countries: a modelling study. Lancet Glob Health. 2025;13:e1517–24. DOIPubMedGoogle Scholar
- Andrews JR, Noubary F, Walensky RP, Cerda R, Losina E, Horsburgh CR. Risk of progression to active tuberculosis following reinfection with Mycobacterium tuberculosis. Clin Infect Dis. 2012;54:784–91. DOIPubMedGoogle Scholar
Figures
Tables
Cite This ArticleOriginal Publication Date: February 27, 2026
Table of Contents – Volume 32, Number 3—March 2026
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Jonathon R. Campbell, McGill University, Office 3D.55, 5252 Blvd de Maisonneuve O, Montreal, QC H4A 3S5, Canada
Top