Volume 31, Number 2—February 2025
Research
Cyclospora Genotypic Variations and Associated Epidemiologic Characteristics, United States, 2018–2021
Cite This Article
Citation for Media
Abstract
Seasonal cyclosporiasis outbreaks occur in the United States every year. To better understand the disease, the Centers for Disease Control and Prevention developed a novel genotyping system that successfully clusters nonclonal eukaryotes. We examined temporal-geographic distributions of Cyclospora cluster consensus genotypes (CCGs) and applied regression analyses to identify correlations between Cyclospora spp. parasites and clinical manifestations or epidemiologic risk factors, using data collected during 2018–2021. No CCG was uniquely associated with or consistently detected in a state during the study, suggesting that cyclosporiasis in the United States is likely caused by frequent parasite introductions. We identified positive associations between infection with C. ashfordi and C. cayetanensis and consumption of specific produce items: cilantro, mango, and onion for C. ashfordi and iceberg lettuce, carrot, and cauliflower for C. cayetanensis. Our findings can guide future research into public health interventions aimed at reducing the burden of cyclosporiasis in the United States.
Cyclospora spp. are foodborne parasites that cause seasonal outbreaks of cyclosporiasis in the United States (1). Cases of this diarrheal disease are often sporadic and geographically dispersed; those characteristics, combined with the lengthy lag period between illness onset and patient interview (typically 4–6 weeks), make it difficult to identify the food vehicles of infection (2). Although cyclosporiasis has been reported year-round in the United States, most cases occur during May–August (3). Molecular typing, in conjunction with epidemiologic methods, has increased our understanding of disease transmission dynamics for other pathogens (4). For cyclosporiasis, the Centers for Disease Control and Prevention (CDC) developed a Cyclospora genotyping system, Cybernetic Clustering Of Nonclonal Eukaryotes (CYCLONE) bioinformatic workflow (5–7), that uses Illumina (https://www.illumina.com) sequence data generated from a set of 8 PCR-amplified Cyclospora genetic markers as input and computes a pairwise distance similarity matrix that is hierarchically clustered to yield clusters of genetically similar samples (8).
Application of CYCLONE previously revealed 2 distinct species of Cyclospora, C. cayetanensis, and C. ashfordi, as agents of cyclosporiasis in the United States (7). Those species are distinguished at the 360i2 nuclear locus and several other loci throughout the Cyclospora genome not included in CYCLONE; alleles are exclusive to each species (7). That study reported geographic and temporal trends during 2018–2020, when C. cayetanensis accounted for an estimated two thirds of documented cyclosporiasis in the United States and was generally a more common cause of illness in northern and midwestern states, whereas Texas and Florida had greater proportions of C. ashfordi infections (7).
The previous observations required deeper analysis, which is the focus of our study. To more precisely track genetic types over different time periods and determine the possibility for locally established foci of infection, we developed a novel approach for cluster categorization, termed cluster-consensus genotypes (CCGs). First, we analyzed observed temporal and geographic patterns by CCG among specimens submitted for Cyclospora genotyping during 2018–2021 to better understand annual variation of Cyclospora CCGs by year and reporting state. Second, we analyzed clinical, biologic, or epidemiologic features that could be associated with the different species of Cyclospora, as has been observed for species of Cryptosporidium (9). We anticipate that our results will serve to bolster our understanding of cyclosporiasis in the United States.
The human subjects coordinator at CDC’s National Center for Emerging and Zoonotic Infectious Diseases reviewed this project and deemed it a nonresearch public health surveillance activity. We conducted the activity consistent with applicable federal law and CDC policy (45 C.F.R. part 46; 21 C.F.R. part 56).
The study is based on 2,770 Cyclospora-positive fecal samples successfully genotyped by CDC during January 2018–December 2021 as available via National Center for Biotechnology Information under BioProject no. PRJNA578931 (5,10,11). We excluded from the analyses 1 fecal sample that was positive for C. henanensis and sequenced as part of the genotyping reference set (7) and samples for which the state of origin could not be ascertained.
Determination of Cyclospora CCGs
Figure 1

Figure 1. Schematic representation of a cluster consensus genotype in study of Cyclospora genotypic variations and associated epidemiologic characteristicsUnited States, 2018–2021. Genotypes are derived from 8...
We submitted sequencing reads to CYCLONE for genotyping and used specimens with haplotypes detected for >5 of the 8 markers to generate genotypes and a pairwise distance matrix in CYCLONE. We clustered the resulting matrix hierarchically to produce a tree, which we dissected into discrete clusters of closely related specimens (8,12). Within each cluster, the genotype found in >50% of specimens became the representative CCG. Because CCGs are an emergent property of the clustering process, the individual genotypes within a cluster might vary slightly from the representative consensus genotype despite sharing most of their core haplotypes. For this study, we identified each CCG with the letter S and a 3-digit number (e.g., S001) (Figure 1). We analyzed proportional distribution of the 2 Cyclospora species on the basis of the submitting state and year of submission. A similar analysis at the CCG level looked at the 5 most frequently detected CCGs within states across the 4 years of the study and presented results as heatmaps. Within our study dataset, some genotyped specimens were previously epidemiologically linked to defined outbreak clusters, but others were not. Therefore, we conducted the CCG analysis first on all available samples (linked and not linked to an outbreak), and then once again only with specimens not linked to epidemiologically identified outbreak clusters, to determine if similar patterns were observed among non–outbreak-related samples.
Associations between Species and Disease Symptoms or Reported Produce Consumption
We filtered the dataset to keep only genotypes with associated epidemiologic data and complete genotype data at the 360i2 locus that was previously described as a species-defining allele for human-infecting Cyclospora (7). When a patient had >1 specimen genotyped, we kept the sample with the most complete genotype. However, if a patient’s samples had discordant genotypes (e.g., for patients who became infected with different species on separate occasions), we excluded all patient samples from the analyses.
We used epidemiologic data from Cyclosporiasis National Hypothesis Generating Questionnaires (CNHGQs), completed by US cyclosporiasis patients during routine public health surveillance, to determine statistical associations between each species of Cyclospora and patient-reported clinical manifestations and produce consumption. The CNHGQ includes questions on patient demographics, state of residence, travel, clinical manifestations, and food consumption in the 2 weeks before symptom onset. We dichotomized responses about symptoms or consumption of food, using yes for yes/maybe responses and no for don’t know/no responses. We used a patient’s home state of residence as a proxy for the site of infection acquisition. Because domestic or international travel affected the validity of this proxy variable, we included travel variables in a regression model described in the next section. The CNHGQ includes food parent variables (e.g., bell pepper); if those elicit an affirmative response, the next question is for specific subset exposures within that parent variable (e.g., red bell pepper, orange bell pepper). We selected food parent variables for analysis and not the subset questions, which frequently had missing responses. Cyclospora outbreak investigations identified whether a person belonged to a specific epidemiologic cluster, in which >2 patients were linked to the same source of infection (i.e., food vehicle, store, or restaurant); such clustering was also factored into the final regression model.
Statistical Analysis
We described continuous variables by mean and SD or median and interquartile range and categorical variables by count and percentage. We assessed potential associations between Cyclospora species and epidemiologic features using Welch 2- sample t-tests for continuous variables and Pearson χ2 or Fisher exact tests for categorical variables. If we could not assume a normal distribution for a continuous variable, we performed a Kruskal-Wallis rank-sum test instead. We presented missing data as the count of patients without a recorded value for a characteristic. We determined p<0.05 as statistically significant.
We used a generalized estimating equation (GEE) with a homogeneous exchangeable/compound symmetric covariance and correlation matrix structure to estimate associations between statistically significant variables from univariate analyses and Cyclospora species. This method enables clustering of outcomes as a result of genetically similar pathogens being connected with a common food vehicle in routine epidemiologic surveillance. Because a previous study (7) observed statistically significant temporal and geographic differences between Cyclospora species, we included both those characteristics in the model. The temporal component comprised 2 variables: year of detection and day of the year (i.e., ordinal date) of symptom onset. Geographic variables included indicators for whether patients lived in Texas or Florida (2 states with higher proportions of C. ashfordi infection in the previous study [7]), whether they traveled out of state, and whether they traveled out of country. We added food and demographic variables to assess if statistically significant differences from bivariate analyses would be maintained after adjusting for covariates. We excluded patients missing any data for selected predictors. We performed all data cleaning, variable transformations, and statistical analyses using R statistical computing and graphics software (The R Project for Statistical Computing, https://www.R-project.org). We used the geepack package (13–15) to fit the GEE and ggplot2 (16) to produce the plots.
Temporal-Geographic Distribution of Cyclospora Species and CCGs
Figure 2

Figure 2. Proportion of Cyclospora cayetanensis and C. ashfordi in 7 states with highest number of specimens in study of Cyclospora ...
Of the 2,770 specimens processed through CYCLONE, we excluded 9 Cyclospora specimens (0.3%): 1 reference isolate from China and 8 specimens for which the state of origin could not be ascertained. The evaluable 2,761 specimens originated from 33 states. The 7 states with the most isolates genotyped over the 4-year study period were New York (n = 651), Texas (n = 551), Florida (n = 222), Illinois (n = 212), Wisconsin (n = 224), Minnesota (n = 204), and Iowa (n = 185) (Figure 2; Appendix).
Overall, 67.1% of samples were C. cayetanensis and 32.9% were C. ashfordi; those percentages varied by state and year (Figure 2). In New York, C. cayetanensis accounted for 65.7%–76.3% of all genotyped specimens. In Iowa, the prevalence of C. cayetanensis fluctuated from 81.5% in 2018 to 96.6% in 2020; no specimens were genotyped in 2021. In Texas, we identified C. ashfordi in 71.4% of specimens submitted in 2020, dropping to 27.3% in 2021. In Florida, the prevalence of C. ashfordi ranged from 15.4% in 2019 to 78.9% in 2020. C. cayetanensis was more prevalent in Illinois, Wisconsin, and Minnesota except for 2019, when the prevalence of C. ashfordi increased to 50.0% in Illinois and 56.7% in Wisconsin.
Figure 3

Figure 3. Heatmaps illustrating the proportions of the top 5 most prevalent CCGs in each of the 7 states with highest number of specimens in study of Cyclospora...
In this study we identified 33 CCGs; 20 belonged to C. cayetanensis and 13 belonged to C. ashfordi (Table 1; Appendix Table 2). The annual distribution of CCGs (Table 1) varied considerably year-to-year. The predominant CCG in 2018 was S029 (27.6%, C. cayetanensis), in 2019 was S004 (17.5%, C. ashfordi), in 2020 was S012 (23.0%, C. cayetanensis), and in 2021 was S012 (19.7%). Of note, CCG S012 represented only 1.4% of specimens in 2018, but its proportion increased in 2020 to 23.0%. Furthermore, we noted high heterogeneity in CCG prevalence within each state over the study period. In some instances, CCGs that were abundant one year were nearly absent in subsequent years (e.g., S029 in Illinois) (Figure 3). Such shifts were less extreme in states like New York, Texas, and Florida that had more cyclosporiasis cases. In general, no specific CCG was uniquely associated with a state, and most CCGs were not detected in similar proportions over the study period. Similarly, no CCG was uniquely associated with a state or year in the analysis of the 2,044 specimens (74.0%) not related to outbreak clusters (Appendix Figure).
Associations between Species and Reported Manifestations or Produce Consumption
Of the 2,761 evaluable genotyped specimens, we excluded 1,045 (37.8%) that lacked an associated CNHGQ record. Seventeen patients had repeat collections, providing 2 Cyclospora specimens each; of those, we excluded 5 patients who exhibited discordant genotypes (10 samples [0.4%]). For the remaining 12 patients, we retained the sample with more complete genotype data (12 exclusions [0.4%]). We also excluded sequences with ambiguous 360i2 data (n = 156 [5.7%]). We used a final sample set of 1,538 patient sequences (55.7% of the evaluable genotyping set) for analyses (n = 214 from 2018, n = 413 from 2019, n = 482 from 2020, n = 429 from 2021). Of the final set, 437 (28.4%) sequences were C. ashfordi and 1,101 (71.6%) were C. cayetanensis.
Most patients were White (n = 1,048 [94%] of 1,113 with race data), and more were female than male (n = 862 [57%] female, n = 650 male [43%], of 1,502 with sex data). The average age was 50.7 years. We detected no statistically significant difference between species groups (p = 0.10). More patients infected with C. ashfordi self-identified as Hispanic (n = 78 [20%]) than those infected with C. cayetanensis (n = 105 [12%]; p<0.001) (Table 2). Eight cyclosporiasis clinical manifestations were documented in the CNHGQ (Table 3). Diarrhea was most commonly reported (n = 1,224 [98%]), followed by abdominal cramps (n = 921 [77%]), fatigue (n = 920 [76%]), weight loss (n = 856 [72%]), nausea (n = 829 [69%]), vomiting (n = 823 [68%]), fever (n = 758 [63%]), and anorexia (n = 751 [63%]). More patients infected with C. cayetanensis than C. ashfordi reported experiencing fatigue (79% vs. 71%; p = 0.003). Among those who responded to all symptom-related questions (n = 1,159), the median number of symptoms in patients with C. cayetanensis was 6 and in patients with C. ashfordi was 5, although this difference was not statistically significant (p = 0.070). Of the 1,416 patients who responded to questions about hospitalization, 81 (5.7%) were hospitalized a median of 3 nights (interquartile range 2–4 nights); maximum stay was 16 nights. A slightly larger percentage of patients with C. ashfordi (n = 30 [7.7%]) were hospitalized than were patients with C. cayetanensis (n = 51 [5.0%]), although the difference was not statistically significant (p = 0.053).
We included 64 produce items for bivariate analysis, although 26.5% of patients (n = 408) did not respond to produce-related questions. A greater percentage of patients infected with C. ashfordi recalled eating cilantro (44% vs. 28%; p<0.001), squash (14% vs. 8.9%; p = 0.010), guacamole (31% vs. 23%; p = 0.003), pico de gallo (32% vs. 25%; p = 0.022), plum (8.8% vs. 4.9%; p = 0.015), onion (49% vs. 41%; p = 0.018), mango (18% vs. 13%; p = 0.024), and lemon or lime (43% vs. 35%; p = 0.014) (Table 4). More patients infected with C. cayetanensis reported consumption of iceberg lettuce (49% vs. 39%; p = 0.001), cauliflower (23% vs. 11%; p<0.001), bagged salad kit (15% vs. 9.4%; p = 0.013), and carrot (30% vs. 23%; p = 0.018).
In addition to covariates for time and geography, we included covariates for ethnicity and produce items with statistically significant results (Table 4) in a GEE model with Cyclospora species as the outcome. We dropped patients with missing covariate values, leaving 908 patients (59%) for analysis (C. ashfordi, n = 277; C. cayetanensis, n = 631). The species proportions remained similar even with such exclusions, suggesting an equitable distribution of missing data across species. The model included year and ordinal date of illness onset to control for temporal variations in species prevalence, but we did not interpret those data for analysis. We detected no multicollinearity among the predictor variables.
Figure 4
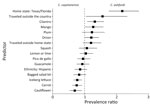
Figure 4. Forest plot presenting prevalence ratio point estimates for all predictors in the generalized estimating equation model in study of Cyclospora ...
Geography and the produce items cilantro, mango, onion, iceberg lettuce, carrot, and cauliflower all had a statistically significant association with Cyclospora species, all else being equal (Figure 4). In patients from Texas or Florida, prevalence of infection with C. ashfordi was 2.18 (95% CI 1.76–2.70) times greater than for C. cayetanensis. Patients reporting international travel were also more frequently infected with C. ashfordi (prevalence ratio [PR] 1.56 [95% CI 1.04–2.34]) than were those who remained in-country. Infections with C. ashfordi were associated with consumption of cilantro (PR 1.32 [95% CI 1.08–1.61]), mango (PR 1.27 [95% CI 1.01–1.59]), and onion (PR 1.45 [95% CI 1.01–1.21]), whereas consumption of iceberg lettuce (PR 0.77 [95% CI 0.65–0.92]), carrot (PR 0.75 [95% CI 0.61–0.92]), and cauliflower (PR 0.69 [95% CI 0.53–0.91]) were significantly associated with C. cayetanensis infections.
This study used a novel genotype designation to understand the genetic diversity and molecular epidemiologic trends of cyclosporiasis in the United States over 4 consecutive years. The data we used are likely representative of the US cyclosporiasis trends given our relatively large and diverse sample size, including samples collected over multiple years.
Although there are annual cyclosporiasis outbreaks in the United States, our understanding of the transmission dynamics of Cyclospora is limited. One such knowledge gap is where produce originally becomes contaminated. One hypothesis suggests that contamination arises from local prevalence or persistence of Cyclospora within the United States (17). Other theories posit that sources of contamination originate outside the United States from repeated introductions such as imported produce, migrant or seasonal farmworkers, travelers carrying the parasite, or other yet-to-be-investigated means (17,18).
This study detected high heterogeneity of CCGs, both over time and by state, findings that may support the hypothesis that cases of cyclosporiasis in the United States are likely caused by frequent new introductions, rather than Cyclospora parasites that persist in the local environment. For example, the high heterogeneity of CCGs observed by state and over time could be attributable to imported produce. Given the globalization of food supplies, produce sold in the United States are imported from many areas, some of which may be endemic for Cyclospora, at different times, which might explain the diversity of CCGs we reported.
We found that New York, Texas, and Florida tended to have higher numbers of reported cyclosporiasis cases than other states. The reasons for this observation are outside the scope of this study but could be attributed to population size or myriad differences related to public health reporting requirements and investigation capacities, access to healthcare, availability of diagnostic testing, or healthcare provider knowledge. For those same reasons, there is an inherent potential for sampling bias to occur in surveillance data. Although those 3 states saw less-pronounced shifts in Cyclospora genetic diversity, we observed no clear dominant or persistent pattern either at the species or CCG level, contrary to what we would expect if the parasite were persisting in the local environment.
The separation of C. cayetanensis into 3 species is a recent taxonomic change (7) and is yet to gain widespread acceptance, as is typical for recent taxonomic revisions, particularly for medically important pathogens. We chose to retain the use of those proposed species’ names for the purposes of this article. Another main finding of this analysis is that the 2 Cyclospora species described previously (7) showed distinct epidemiologic characteristics, potentially underpinning some presently unknown biologic differences between C. cayetanensis and C. ashfordi and providing further evidence in support of their taxonomic separation. Certain produce items were more commonly associated with C. cayetanensis and others with C. ashfordi. Because numerous specimens were collected during outbreak investigations, it is likely that related specimens will be found within clusters that are determined through epidemiologic analysis, with one food source serving as a common link. The occurrence of such clustering can create spurious associations; we used a multivariate GEE model to establish the relationship between predictor variables and Cyclospora species while considering the correlation between specimens within the same cluster (19). To account for spatiotemporal variability in CCG distribution, the model included covariates for geography and year. Our findings demonstrated that associations between some produce items and species remained statistically significant even after adjusting for clustering and spatiotemporal variance. However, certain produce items may be underreported because they do not constitute a major ingredient in a dish and persons may not recall consuming them; herbs are a prime example. In addition, because many fresh produce items are consumed in mixtures such as bagged salad mixes, guacamole, or pico de gallo, it can be difficult to pinpoint the true vehicles or predictors for Cyclospora. Despite those drawbacks, our findings identified several produce items of interest, and determining if there are factors in growing, harvesting, handling, or storage conditions of those produce items that may increase the likelihood of Cyclospora contamination is an area for further research.
Given that CCGs are an emergent property of probabilistic genetic clustering and the genetic clusters themselves are composed of similar but not always identical genotypes (5,6), the CCGs reported here may change in future studies. For example, a set of isolates may always genetically cluster together, but their CCG may change if isolates added or removed from the dataset cause the consensus genotype of the genetic cluster to change. Furthermore, the CCGs we described were created using 8 genetic markers; future addition of genotyping markers will increase the discriminatory capacity and long-term stability of CCGs but will also lead to the redefinition of genetic clusters. For those reasons, the CCGs we identified are robust for this study but may evolve when using either additional markers or other datasets, and the produce relationships identified in these analyses may change in future analyses. Overall, this study provides a foundation for improving our understanding of cyclosporiasis epidemiology in the United States.
The CNHGQ surveys were administered to patients after a confirmed laboratory diagnosis of cyclosporiasis, typically many days after infection has occurred. Therefore, the data may be affected by recall or symptom-associated biases (20), missing data, discrepancies, or errors. For this study, more than one third of samples from the genotyping dataset lacked corresponding CNHGQ data. Given their contributions to this type of molecular epidemiology study, having more complete CNHGQ information should be a focus for future work.
This study highlights several opportunities for future work. First, the CCGs were determined using at most 8 genetic markers that may not capture differences in other regions of the Cyclospora genome. Therefore, including additional genotyping markers could enhance the use of CCGs for molecular epidemiologic studies. Second, there is a need to collect and sequence Cyclospora samples from endemic areas because those data will enhance the understanding of the genetic diversity of Cyclospora and CCGs over space and time, and their genetic information may improve the stability of CCGs and genotyping methods.
Understanding food distribution networks and their variations can offer valuable insights into why specific species and CCGs appear in certain locations during particular times of year; that knowledge could shed light on whether CCGs are associated with the origin, processing or distribution of produce. Continued genotyping as part of ongoing, routine cyclosporiasis surveillance will bolster knowledge on temporal patterns of Cyclospora. Overall, such studies promise to improve cyclosporiasis outbreak investigations, potentially enabling investigators to trace the origins of Cyclospora-contaminated produce with heightened precision and fostering the development of prevention and control programs.
Acknowledgments
We thank the state and local health departments who worked diligently to collect epidemiological data and stool specimens from cyclosporiasis cases and provide those data to CDC. We thank Yvonne Qvarnstrom, Katelyn Houghton, Travis Richins, Anna Peterson, Lauren Ahart, Cody Bennett, Shannon Casillas, and Marion Rice, whose labors also contributed to the epidemiological data that made this study possible.
Mr. Shen is a researcher, as part of the Oak Ridge Institute for Science and Education (ORISE) fellowship program, in the Division of Parasitic Diseases and Malaria, National Center for Emerging and Zoonotic Infectious Diseases, Centers for Disease Control and Prevention, Atlanta, Georgia, USA. His research interests include the epidemiology and prevention of zoonotic and human infectious diseases.
References
- Casillas SM, Bennett C, Straily A. Notes from the field: multiple cyclosporiasis outbreaks—United States, 2018. MMWR Morb Mortal Wkly Rep. 2018;67:1101–2. DOIPubMedGoogle Scholar
- Casillas SM, Hall RL, Herwaldt BL. Cyclosporiasis Surveillance - United States, 2011-2015. MMWR Surveill Summ. 2019;68:1–16. DOIPubMedGoogle Scholar
- Centers for Disease Control and Prevention. Domestically acquired cases of cyclosporiasis — United States, May–August 2022. 2022 [cited 2023 Mar 27]. https://web.archive.org/web/20230328230137/https://www.cdc.gov/parasites/cyclosporiasis/outbreaks/2022/seasonal/index.html
- Sulaiman IM, Xiao L, Yang C, Escalante L, Moore A, Beard CB, et al. Differentiating human from animal isolates of Cryptosporidium parvum. Emerg Infect Dis. 1998;4:681–5. DOIPubMedGoogle Scholar
- Nascimento FS, Barratt J, Houghton K, Plucinski M, Kelley J, Casillas S, et al. Evaluation of an ensemble-based distance statistic for clustering MLST datasets using epidemiologically defined clusters of cyclosporiasis. Epidemiol Infect. 2020;148:
e172 . DOIPubMedGoogle Scholar - Barratt JLN, Park S, Nascimento FS, Hofstetter J, Plucinski M, Casillas S, et al. Genotyping genetically heterogeneous Cyclospora cayetanensis infections to complement epidemiological case linkage. Parasitology. 2019;146:1275–83. DOIPubMedGoogle Scholar
- Barratt JLN, Shen J, Houghton K, Richins T, Sapp SGH, Cama V, et al. Cyclospora cayetanensis comprises at least 3 species that cause human cyclosporiasis. Parasitology. 2023;150:269–85. DOIPubMedGoogle Scholar
- Jacobson D, Barratt J. Optimizing hierarchical tree dissection parameters using historic epidemiologic data as ‘ground truth’. PLoS One. 2023;18:
e0282154 . DOIPubMedGoogle Scholar - Cama VA, Ross JM, Crawford S, Kawai V, Chavez-Valdez R, Vargas D, et al. Differences in clinical manifestations among Cryptosporidium species and subtypes in HIV-infected persons. J Infect Dis. 2007;196:684–91. DOIPubMedGoogle Scholar
- Barratt J, Houghton K, Richins T, Straily A, Threlkel R, Bera B, et al. Investigation of US Cyclospora cayetanensis outbreaks in 2019 and evaluation of an improved Cyclospora genotyping system against 2019 cyclosporiasis outbreak clusters. Epidemiol Infect. 2021;149:
e214 . DOIPubMedGoogle Scholar - Ahart L, Jacobson D, Rice M, Richins T, Peterson A, Zheng Y, et al. Retrospective evaluation of an integrated molecular-epidemiological approach to cyclosporiasis outbreak investigations - United States, 2021. Epidemiol Infect. 2023;151:
e131 . DOIPubMedGoogle Scholar - Barratt JLN, Plucinski MM. Epidemiologic utility of a framework for partition number selection when dissecting hierarchically clustered genetic data evaluated on the intestinal parasite Cyclospora cayetanensis. Am J Epidemiol. 2023;192:772–81. DOIPubMedGoogle Scholar
- Yan J. geepack: yet another package for generalized estimating equations. R J. 2002;2:12–4.
- Yan J, Fine J. Estimating equations for association structures. Stat Med. 2004;23:859–74, discussion 875–7, 879–80.
- Halekoh U, Højsgaard S, Yan J. The R package geepack for generalized estimating equations. J Stat Softw. 2005;15:1–11.
- Wickham H. ggplot2: Elegant graphics for data analysis. New York: Springer-Verlag; 2016.
- Chacin-Bonilla L, Santin M. Cyclospora cayetanensis infection in developed countries: potential endemic foci? Microorganisms. 2023;11:540. DOIPubMedGoogle Scholar
- National Advisory Committee on Microbiological Criteria for Foods (NACMCF). Response to questions posed by the Food and Drug Administration (FDA): Cyclospora cayetanensis in produce. 2023. [cited 2023 Nov 15] https://www.fsis.usda.gov/sites/default/files/media_file/documents/NACMCF_Cyclospora_Report_2023_Final.pdf
- Zeger SL, Liang KY, Albert PS. Models for longitudinal data: a generalized estimating equation approach. Biometrics. 1988;44:1049–60. DOIPubMedGoogle Scholar
- Raphael K. Recall bias: a proposal for assessment and control. Int J Epidemiol. 1987;16:167–70. DOIPubMedGoogle Scholar
Figures
Tables
Cite This ArticleOriginal Publication Date: January 22, 2025
1These senior authors were co–principal investigators.
Table of Contents – Volume 31, Number 2—February 2025
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Anne Straily, Centers for Disease Control and Prevention, 1600 Clifton Rd NE, Mailstop H16-4, Atlanta, GA 30329-4018, USA
Top